Dr. Allen Ali Nasseh knows that the phases of endodontic treatment need both positive and negative pressure irrigation. See how the TotalVac Irrigation System gets the job done, with one single system.
Dr. Allen Ali Nasseh explores whether the positive and negative pressure needs of clinicians can be met with a simple and inexpensive device
During a conventional root canal procedure, the operator must manage the multiple liquids used to facilitate the access, chemomechanical instrumentation, and final obturation steps of the procedure. These liquids are used at each phase of the procedure and have specific functions.1 The access preparation phase requires water coolant spray from high- speed handpieces. Chemomechanical instrumentation requires positive pressure irrigation of disinfectants and chelators in the coronal and apical segments of the root canal, and finally, a bout of negative pressure irrigation is used by some clinicians to safely run a high-volume of disinfectant and chelating agents at the end of the procedure for enhanced apical cleaning prior to obturation.1-3 During each phase, multiple solutions including water, sodium hypochlorite, chelators, and lubricants help facilitate the process of root canal therapy and allow us to get rid of the infected pulp and biofilm, clear dentinal debris, and prepare a clean root canal surface ready for obturation.2
To manage these fluids, suction (negative pressure) is required to clear excess fluids and macro debris from the area. The operator, generally aided by a dental assistant, starts the procedure by a sequence of high-speed evacuation to remove the water coolant from the area after it is expressed from the handpiece, then switch to surgical suction to manage the debris and added irrigants during root canal instrumentation, and finally switch to another device for negative pressure suction at the end of instrumentation.3 These three phases often require three separate HVE suction outlets from the operatory unit with three separate components and a complicated workflow.

Recently, a novel modular device has been developed by the author that may help address the clinical needs for positive and negative pressure irrigation during these three phases of treatment through the application of a single system. The TotalVac Irrigation System (Brasseler USA®, Savannah, Georgia) is a disposable kit that allows the operator to use the aforementioned positive and negative pressure application of fluids during the root canal procedure through modular use of its components (Figure 1). The kit consists of three main parts:
- High-Speed Evacuation Tip
- The Surgical Suction Adaptor
- The Negative Pressure Tubing
High-Volume Evacuation
This is the most intuitive component of the system. It duplicates the conventional high-volume evacuation; however, the nozzle size is in-between a large high-volume evacuation tip and a surgical suction tip. Therefore, this tip can generally be used for both applications during access preparation and normal evacuation of fluids during instrumentation. This item requires a single suction inlet from the operatory unit (Figure 2).

Surgical Suction Adaptor
If more precise suction application is needed than that provided by the High-Volume Evacuator, a Surgical Suction Adaptor can be fitted to the High-Volume Evacuator Tip, transforming it into a surgical suction (Figure 3). This allows an efficient conversion of high-speed evacuation to surgical suction, and vice versa. The dental assistant can merely take on-and-off this adaptor to switch between two types of suction instead of replacing the entire suction tip or requiring two separate HVE inlets with two separate suction tips on the operatory unit.
Negative Pressure Tubing
While high-volume evacuator and surgical suction are used by all clinicians doing endodontic therapy, applying suction capability closer to the treatment site without the aid of an assistant may be necessary in some clinical settings where a dental assistant may not be available during this phase of the procedure. This is common in dental school/residency and some private practice settings. Furthermore, some astute clinicians prefer using a large volume of irrigation inside the root canal with the safety of negative pressure techniques instead of mere positive pressure irrigation at the end of instrumentation.3 The purpose of the TotalVac Tubing is to address both of these needs through its modular design (Figure 4). The HVE fitting end of the tubing can be connected directly to an available HVE inlet in the operatory, or if an extra inlet is not available, the HVE fitting can be attached directly to the Surgical Suction Adaptor and connected to the High-Speed Evacuation Tip. This gives the operator the option of using only a single HVE inlet for all the various phases and applications of this device from access to obturation by using different configurations of tips in a modular manner. However, direct connection of the HVE connection into an available HVE inlet in the operatory is generally the most convenient configuration of this tubing according to the author.
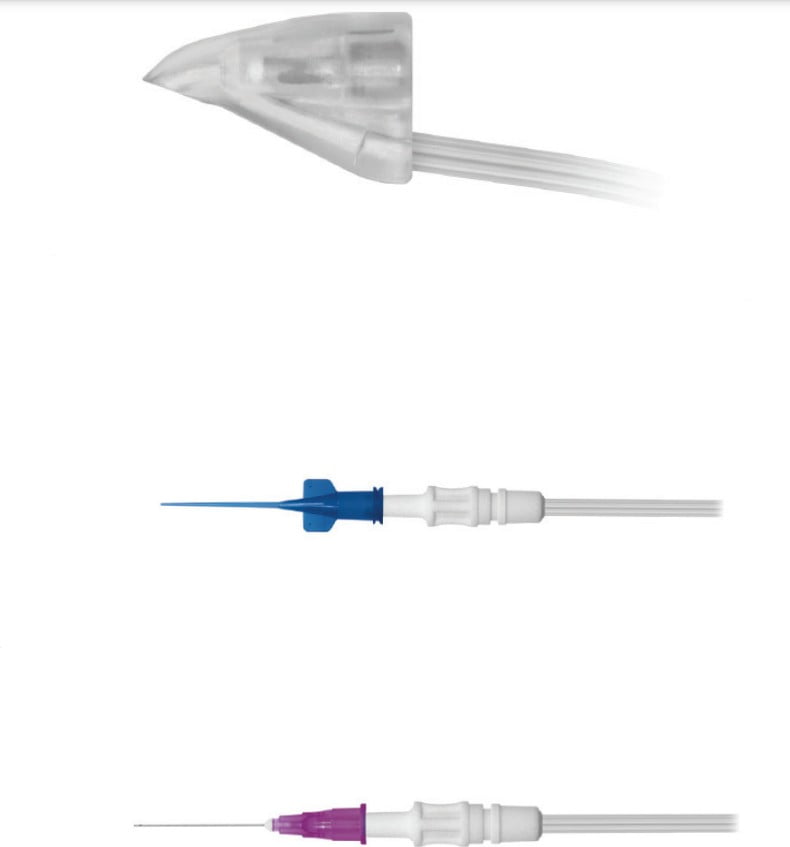
The TotalVac Tubing bifurcates in two separate suction tubes. One end of tubing is connected to the manifold, a sleeve that houses a short Luer Lock needle that connects to the irrigation syringe for delivery of irrigation solution with simultaneous suction of excess fluid (Figure 5). The other end accommodates a handpiece that can be fitted with conventional Luer Lock delivery tips or needles to allow suction inside the root canal (Figure 6). The kit is supplied with a flexible plastic suction tip for average-size canals and a 30 gauge close-ended, side-vented needle that can be used for thinner canals. The same 30 gauge needle can also be used for positive pressure irrigation in combination with the plastic manifold at the other end of the TotalVac Tubing (Figure 7).
However, in negative pressure applications, it’s important to recognize that the use of this macro and micro level of suction deep in the root canal should really be limited to the end of instrumentation and after all the large pulp and dentinal debris have been removed from the canal to avoid clogging of the applicators tips.
The TotalVac Tubing assembly can operate under four distinct modes of operation. These modes are used based on the stage of chemomechanical instrumentation (early or late) or the need for negative or positive pressure during irrigation (operator preference). Not all four modes are required during a single procedure, and the modularity of this device makes it possible for each operator to choose the modes he/she prefers for positive or negative pressure irrigation throughout the procedure.
The four possible modes of application consist of two positive pressure (irrigation) modes and two negative pressure (suction) modes.

Coronal Irrigation (Mode 1)
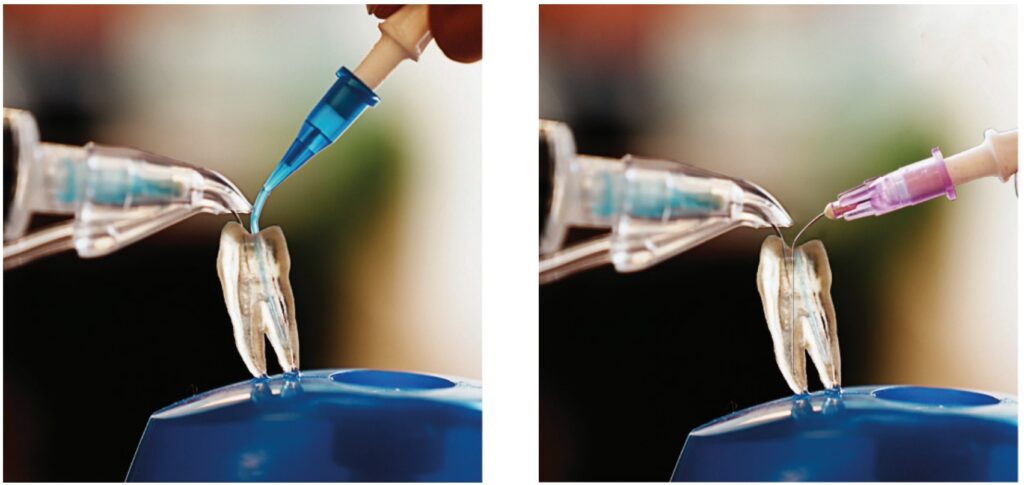
The short needle in the manifold is connected to your irrigation solution of choice, and irrigation is deposited into the chamber while excess is suctioned up through the manifold (Figure 8). This allows single-handed operation of the syringe combining irrigation with suction. The manifold suction assembly should be kept very close to the cavosurface area of the access to allow suctioning of the excess fluid. (Note: The use of a caulking material to achieve secondary isolation of a fluid tight seal around the rubber dam is generally recommended prior to all root canal therapy.) Since the manifold needle is short and does not reach in the depths of the canal, this form of irrigation allows effective irrigation in only the coronal half of the root canal. This mode can be combined with the handpiece applicator to achieve high-volume negative pressure toward the end of the procedure (Modes 3 and 4).
Apical Irrigation (Mode 2)
To achieve deeper irrigation using this one-handed technique, the short needle can be removed from the manifold and replaced with the 30 gauge needle. After threading the needle through the manifold, the tip can be bent 90 degrees for better access to the canal orifice (Figure 9). The needle can protrude up to 17 mm from the manifold reaching deep in the root canal. Longer needles are available for longer roots if deeper insertion is desired. Since the manifold has to be close to the cavosurface area of the access to achieve effective suction of excess fluids in the canal, it’s recommended to continue to use the Coronal Irrigation needle (Mode 1) until working length has been established and confirmed, and the canal has been enlarged adequately to accommodate the 30 gauge needle to a depth of 17 mm. Otherwise, inadequate insertion depth will not allow the simultaneous suction through the manifold as the suction nozzle won’t be close enough to the cavosurface area to capture the fluids. Establishing working length and some initial enlargement first also allows the operator to avoid accidental insertion of the tip beyond the apex.
Macro Suction (Mode 3)
After instrumentation is complete using positive pressure irrigation and all macro debris is removed, the canal is ready for obturation. At this point, many operators may elect to run a high-volume of disinfectant safely in the canal to remove any remnant tissue at the apical third of the canal.3 Here, the goal is to place a suction tube deep in the canal while irrigation solution is added coronally (Figure 10). The negative pressure created apically by suction will pull the coronally deposited fluids apically toward the suction tip and clear up the suction. This allows a large volume to flow through the canal without the risk of extrusion. In this mode, the operator may insert the plastic dispensing tip on the handpiece to achieve suction deep in the canal while the assistant is depositing the irrigant on top with the aid of the coronal suction assembly (Mode 1). Therefore, Mode 3 can be summarized with the simultaneous use of the plastic suction tip on the handpiece with Mode 1. It’s important to use this mode toward the end of instrumentation to avoid clogging of the tip of the plastic suction tip with large tissue and debris remaining in the canal.
Micro Suction (Mode 4)
This mode of operation is identical to the Macro Suction (Mode 3), except that instead of using the plastic suction tip on the handpiece, the thinner 30 gauge needle is used on the handpiece in order to achieve an even deeper depth of insertion in thinner canals (Figure 11). The insertion depth is limited to inside the root canal and should only be used at the very end of the procedure after all large pulp debris and dentinal chips have already been removed to avoid clogging of the small needle port with large debris in this negative pressure mode.
Clinical Adaptation
Most clinicians will find their own preference for the combined use of positive or negative pressure irrigation when using this device. Most people will use the high-speed evacuation and adaptor for most suction needs and use the 30 gauge needle for conventional positive pressure irrigation on a syringe while using the plastic suction tip and the short needle on the manifold (as preassembled in the kit) for negative pressure irrigation toward the end of the procedure prior to obturation. Furthermore, having the plastic tip available during the procedure helps manage the fluid levels in the chamber and dry the canal from fluid during apex location stage for a more accurate measurement or drying the canals just prior to obturation.
The most practical clinical tip for using this system involves connecting the negative pressure tubing to a separate HVE inlet and resting the coronal suction manifold and short dispensing needle along with the handpiece and the plastic dispensing tip on a waterproof apron or tray on or near the patient’s chest for quick access. Then use the system for positive pressure irrigation at the beginning of the procedure and negative pressure at the end of the procedure. The plastic suction tubing can be used throughout the procedure to control the fluids in the chamber and canal with precision.
Limitations
Like every clinical device, this device has its limitations too. The depth of insertion of needle in Mode 1 is limited to the coronal area of the root and chamber or to 17 mm at the longest end in combination with the 30 gauge needle (Mode 2). Even though most clinicians limit their needle insertion in the canal to these same average depths, some operators may prefer needle insertion down to 1 mm short of the apex. In longer roots, a different length needle should then be used than that which is provided in the kit. Alternatively, normal positive irrigation with the 30 gauge needle and conventional syringe can be used, and this device’s use could be limited to its negative pressure and micro suction applications throughout the procedure. Another challenge is the use of multiple syringes with different solutions during Modes 1 and 2, which would require removing and reconnecting different solution syringes to the manifold using the same syringe tip, which may feel cumbersome if repeated multiple times.4 The most practical solution is combining TotalVac with and all-in-one irrigation solution such as Triton™ (Brasseler USA®, Savannah, Georgia) that can bypass the need for multiple syringes by combining all required solutions in one syringe. Triton contains sodium hypochlorite, chelating agents as well as surfactants and lubricants, all in a single syringe and can provide additional efficiency of using a single syringe of solution from the beginning to the end of the procedure in conjunction with this device.5
TotalVac is a modular irrigation device that has been designed to address the positive pressure and negative pressure irrigation needs of clinicians during root canal therapy.
Advantages
The most important advantage of this system is that it’s more versatile than other similar negative pressure devices in the past and can achieve the same negative pressure principles plus additional modes — all at a much lower cost than alternative options on the market. The system allows each operator to use it based on his/her own needs and priorities. Some operators may use all four modes, some may only use it for modes 1 and 2, and others may just apply deep negative pressure disinfection prior to obturation. Lastly, some may only want to use the plastic dispensing tip to manage the level of fluids in the canal with precision during chemomechanical instrumentation, apex location, and obturation while using conventional syringe irrigation.
Conclusion
TotalVac is a modular irrigation device that has been designed to address the positive pressure and negative pressure irrigation needs of clinicians during root canal therapy. This system can be customized based on each operator’s preference for positive or negative pressure irrigation at different phases of treatment through four modes of operation. Each clinician will find the optimum workflow that works best for him/her after understanding the various applications of this device.
While the system has some limitations, its relatively low cost and versatility can make it a practical solution for most irrigation needs chairside.
Besides the TotalVac Irrigation System, Dr. Brett E. Gilbert answers some questions about other advances in apical negative pressure irrigation. Read his article here: https://endopracticeus.com/industry-news/apical-negative-pressure-irrigation-advances-endodontic-treatment/
 Allen Ali Nasseh, DDS, MMSc, received his dental degree from Northwestern University Dental School in Chicago, Illinois, in 1994 and completed his postdoctoral endodontic training at Harvard School of Dental Medicine in 1997, where he also received a Master of Medical Sciences (MMSc) degree in the area of bone physiology. He has been a clinical instructor and lecturer in the postdoctoral endodontic program at Harvard School of Dental Medicine since 1997 and the Alumni Editor of Harvard Dental Bulletin. Dr. Nasseh is the endodontic advisor to several educational groups and study clubs and is endodontic editor to several peer-reviewed journals and periodicals. He has published numerous articles and lectures extensively both nationally and internationally in surgical and nonsurgical endodontic topics. Dr. Nasseh is in solo private practice (MSEndo.com) in downtown Boston, Massachusetts. Dr. Nasseh is the President and Chief Executive Officer for the endodontic education company Real World Endo® (RealWorldEndo.com).
Allen Ali Nasseh, DDS, MMSc, received his dental degree from Northwestern University Dental School in Chicago, Illinois, in 1994 and completed his postdoctoral endodontic training at Harvard School of Dental Medicine in 1997, where he also received a Master of Medical Sciences (MMSc) degree in the area of bone physiology. He has been a clinical instructor and lecturer in the postdoctoral endodontic program at Harvard School of Dental Medicine since 1997 and the Alumni Editor of Harvard Dental Bulletin. Dr. Nasseh is the endodontic advisor to several educational groups and study clubs and is endodontic editor to several peer-reviewed journals and periodicals. He has published numerous articles and lectures extensively both nationally and internationally in surgical and nonsurgical endodontic topics. Dr. Nasseh is in solo private practice (MSEndo.com) in downtown Boston, Massachusetts. Dr. Nasseh is the President and Chief Executive Officer for the endodontic education company Real World Endo® (RealWorldEndo.com).
Disclosure: Dr. Nasseh is a speaker and key opinion leader for Brasseler USA® and has received compensation for lecture presentations showcasing the company’s bioceramics.
- Konstantinidi E, Psimma Z, Chávez de Paz LE, Boutsioukis C. Apical negative pressure irrigation versus syringe irrigation: a systematic review of cleaning and disinfection of the root canal system. Int Endod J. 2017;50(11):1034-1054.
- Basrani, B. And Haapasalo, M. Update on Endodontic Irrigating Solutions. Endod Topics. 2012,27(1):74-102.
- Kungwani ML, Prasad KP, Khiyani TS. Comparison of the cleaning efficacy of EndoVac with conventional irrigation needles in debris removal from root canal. An in-vivo study. J Conserve Dent. 2014;17(4):374-378.
- Grawehr M, Sener B, Waltimo T, Zehnder M. Interactions of Ethylenediamine Tetraacetic Acid with Sodium Hypochlorite in aqueous solution. Int Endod J. 2003; 36(6):411-415.
- Nasseh AA. Streamlining Effective Irrigation. Endodontic Practice US. 2022;15:(3) 10-12.
Stay Relevant With Endodontic Practice US
Join our email list for CE courses and webinars, articles and more..
