Editors Intro: This research delves into the differences between the single gutta-percha cone technique and GuttaCore.
Drs. Juan Antonio Araujo, Carlos Cantarini, Viviana Han, and Fernando Goldberg study different techniques for obturating lateral canals in premolars
Abstract
Objective
To compare the ability of the single gutta-percha cone technique and the GuttaCore® system (Dentsply Sirona, Ballaigues, Switzerland) for the obturation of simulated lateral canals in extracted human premolars.
Materials and methods
The root canals of 26 extracted human mandibular premolars were instrumented with WaveOne® primary (Dentsply Sirona) and irrigated with NaOCl 2.5%. Then three simulated lateral canals were drilled in the mesial surface of the roots, one in each third, using an Engine Reamer No. 15. To mimic the pulpal tissue, a colored paraffin gel was injected inside the root canals. To mimic the periodontal tissue, the roots were covered with rubber foam and Teflon™. Afterward, the root canals were instrumented with WaveOne large and irrigated with NaOCl 2.5%. Then, EDTAC and NaOCl were activated with an EndoActivator® (Dentspy Sirona). The teeth were divided in two groups of 13 specimens each.
- Group 1: obturated with a WaveOne large single cone.
- Group 2: obturated with a GuttaCore®
In both groups, AH Plus® (Dentsply DeTrey GmbH, Konstanz, Germany) was used as a sealer. Digital X-rays were taken in the buccolingual direction, and the lateral canals were categorized as not filled, partially filled, and totally filled. The specimens were cleared and photographed in order to know the type of material located inside the simulated lateral canals. Data between techniques in each third were statistically analyzed using the Mann-Whitney test. For the comparison between thirds in each technique, the Friedman test was used.
Results
In the postoperative digital images, the comparison within the same third of the root canals showed no statistical significant differences between techniques (P >0.05).
The comparison between thirds in the same technique showed that, in group 1, statistically significant differences between the cervical and the other thirds (P <0.05); but in group 2, not statistically significant differences were detected between thirds (P >0.05). The cleared specimens showed the presence of sealer in all the simulated lateral canals totally obturated from group 1, while in group 2, the cervical third showed 5 with sealer and 5 with gutta-percha, in the middle third 5 and 8, and in the apical third 7 and 5, respectively.
Conclusion
With both techniques, the simulated lateral canals were frequently filled, noticing with GuttaCore a tendency to obturate the lateral canals with gutta percha.
Objective
The objective of this study was to compare the ability of the single gutta-percha cone technique and the GuttaCore system for the obturation of simulated lateral canals in extracted human premolars.
Introduction
The cleaning, shaping, and adequate obturation of the root canal system represents a fundamental objective to achieving success in endodontic therapy. The intricate anatomy of the canals, represented by isthmus, irregularities, and lateral and accessory canals becomes a challenge at every endodontic procedure.
Lateral and accessory canals play an important role because they connect the main root canal with the periodontal ligament. Pulp necrosis and simultaneous bacterial invasion found in lateral canals of great diameters become a pathway to invade the periodontal ligament and generate a lateral lesion.1 De Deus2 cites the presence of lateral canals in 27.4% of 1,140 analyzed teeth. Among those, 17% were detected in the apical third, 8.8% in the middle third, and 1.6% in the coronal third of the root.
In canals with necrotic pulp, the organic debris and bacteria along with their byproducts are difficult to remove from the lateral and accessory canals through instrumentation and irrigation.3 In this respect, the obturation of the lateral canals during an endodontic treatment seals the passage of microorganisms toward the periodontal ligament allowing for a favorable environment for tissue repair.4-6
Different procedures were used to evaluate the behavior of the obturation techniques with respect to the lateral and accessory canals. In this study, the use of human teeth with simulated lateral canals, drilled in the three thirds of the root, allows a more accurate study than using plastic or acrylic models.7 Moreover, these models generally have lateral canals with a greater diameter that do not represent a truthful reality.8
The obturation with a single gutta-percha cone and sealer is one of the techniques universally utilized by general dentists, while the thermoplasticized gutta-percha techniques are generally used by endodontists. Within the thermoplasticized techniques, the GuttaCore® system (Dentsply Sirona, Ballaigues, Switzerland) presents the same principles as its predecessor Thermafil® (Dentsply Maillefer, Ballaigues, Switzerland) with a few modifications. Its core carrier, easy to remove (partial or total), is made from a cross-linked thermoset elastomer of gutta percha.9 The gutta percha that covers the core is high in viscosity, flowability, and adhesion, and its melting temperature is 56°C.9 GuttaCore is manufactured according to the calibers and tapers of the WaveOne system.
The purpose of this study was to evaluate the capacity of the single cone and GuttaCore techniques for the obturation of the simulated lateral canals.
Materials and methods
Twenty-six human inferior premolars with one root canal and a mature apex were used in this study. All teeth were submerged in a hypochlorite solution at 5.25% for 24 hours and then washed with tap water for 15 minutes. Radiographs in buccolingual and mesiodistal directions were taken to evaluate the root canal anatomy. Conventional access preparations were prepared, and the canal length was visually established by placing a No. 15 file in each root canal until it was seen emerging through the apical foramen. The working length was determined by subtracting 1 mm from the total canal length. The root canals were instrumented with WaveOne primary files up to the working length. For this procedure, a motor XSmart™ Plus was utilized following the manufacturer’s instructions. During the instrumentation, the root canals were irrigated with 2 ml of 2.5% sodium hypochlorite solution using a 25 Gx1″ needle (Terumo, Leuven, Belgium).
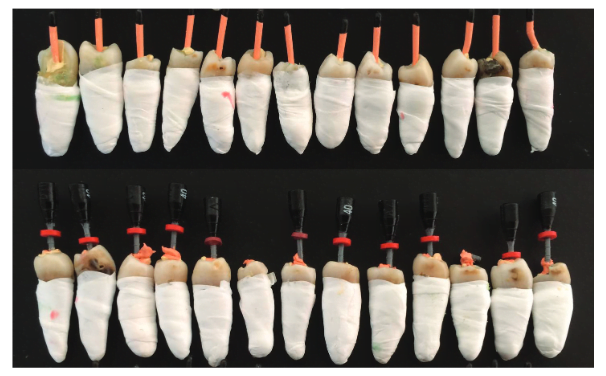
Afterward, three simulated lateral canals were drilled on the mesial surface of the root (one on each third) by using an Engine Reamer No. 15. To verify canal patency, a K-File No. 10 was introduced in the simulated lateral canals and a K-File No. 25 in the root canal that should be blocked by the previous instrument. Consequently, to simulate the pulp, a paraffin gel (Creativa, Décimo Arte SRL, Buenos Aires, Argentina) colored with a bright green paint (Alba Artistica SA, Buenos Aires, Argentina) was injected inside the root canal (Figure 1). The extrusion of the colored gel through the apical foramen and simulated lateral canals was visually checked to confirm their complete filling. Then the external surfaces of the root were cleaned with gauze. The roots were covered with a thin film of foam rubber and Teflon tape to mimic the periodontal ligament. Subsequently, the root canals were instrumented again with WaveOne large files up to the working length using a XSmart Plus motor following the manufacturer’s instructions. At the completion of instrumentation, 2 ml of 2.5% sodium hypochlorite solution was used for irrigation. To control the penetration of the solution, a silicone stop was placed on the needle so that it was always inserted 3 mm from the working length. Once the instrumentation was finished, EDTA (Farmadental, Buenos Aires, Argentina) was activated for 1 minute with an EndoActivator and a large activator tip (Dentsply Sirona) at 10.000 cpm and then 2.5% sodium hypochlorite solution activated during 30 seconds with the same device. The root canals were dried with large WaveOne paper points (Dentsply Sirona), and the 26 teeth were randomly separated into two equal groups of 13 (Figure 2).
- Group I (N = 13): The root canals were obturated with a large WaveOne single gutta-percha cones (Dentsply Sirona).
- Group 2(N = 13): The root canals were filled with large GuttaCore (Dentsply Sirona) softened by a ThermaPrep 2 Oven® (Dentsply Sirona, Ballaigues, Switzerland).
In both groups, AH Plus (Dentsply DeTrey GmbH, Konstanz, Germany) was used as a root canal sealer. The sealer was mixed according to manufacturer’s instructions and then applied by coating the canal walls using a No. 25 file.
Postoperative digital images were taken in buccolingual direction and projected in order to evaluate the number of obturated lateral canals, which were categorized as follows: not obturated, partially obturated, and totally obturated.
Samples were then decalcified in 5% nitric acid, dehydrated in ascending concentrations of alcohol (80%, 90%, and 100%), and cleared using methyl salicylate.10
To compare both techniques within each third of the roots, the Mann-Whitney test was used. For the comparison between the thirds of the roots of each technique, the Friedman test was utilized.
Results
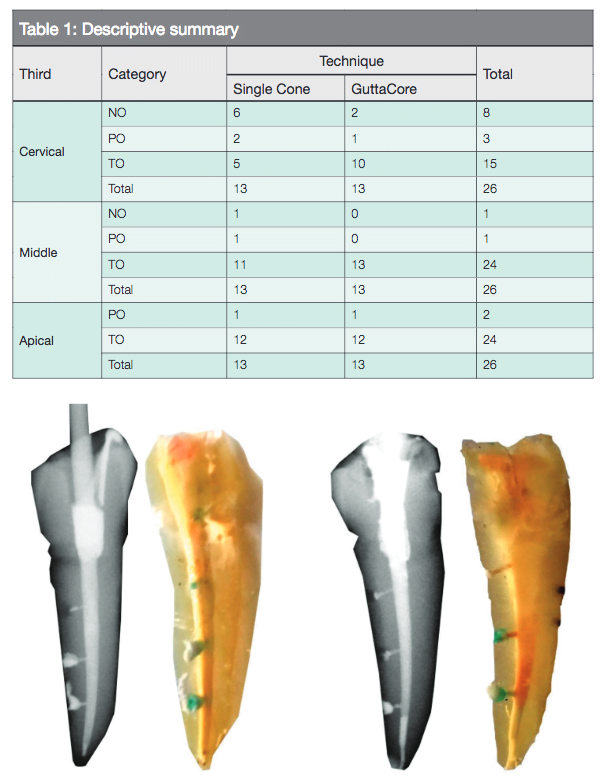
The results can be observed on Table 1.
In the postoperative digital images, the comparison within the same third of the root canals showed no statistical significant differences between techniques (P >0.05).
The comparison between thirds in the same technique showed that, in group 1, statistical significant differences between the cervical and the other thirds (P <0.05); but in group 2, not statistically significant differences were detected between thirds (P >0.05).
In group 1, the evaluation of the cleared specimens demonstrated that, in the 28 simulated lateral canals completely obturated, the presence of sealer inside them. In group 2, of the 35 filled lateral canals, 5 were obturated with sealer in the cervical third and 5 with gutta-percha, 5 and 8 in the middle third, and 7 and 5 in the apical third, respectively (Figures 3 and 4).

Discussion
The presence of lateral canals in teeth with necrotic pulp may cause lateral periodontal lesions. The instrumentation and irrigation of the root canal along with an adequate tridimensional obturation generally leads to the repair of the pathology with new bone formation.
While some studies demonstrate that the use of mechanized systems of instrumentation allows clinicians to obtain an adequate preparation for the adjustment of the single cone, other publications point out the lack of correlation between instruments and cones within the same system and between instrumented canals and gutta-percha cones, respectively.11-13
Several authors highlight the importance of obturating lateral canals with the objective of promoting repair.4-6 Numerous publications demonstrate that the thermoplasticized techniques favor the obturation of the lateral and accessory canals.8,14,15
It is important to mention, as Gulgen-Filho, et al.,16 and Karabucak, et al.,17 that the different brands of gutta percha with diverse formulas behave in different manners due to the variations in fluidity. The use of thermoplasticized gutta-percha techniques generally allow the filling of the lateral canals with gutta percha; on the other hand, with the lateral condensation technique, the obturation of the lateral canals was achieved only with sealer.14,18,19
In this study, by using the single-cone technique and AH Plus sealer, 28 simulated lateral canals that were totally obturated were found to be filled with sealer. In the GuttaCore technique, within the 35 simulated lateral canals, 17 were obturated with sealer and 18 with gutta percha.
Comparative studies related to the obturation of root canals demonstrated that when GuttaCore was used, the mass of the gutta percha filled the irregularities more satisfactorily than the single-cone technique, which left a thinner film of sealer in the interphase.20,21 The cleared specimens allow for the distinguishing of the type of material that fills the simulated lateral canals.
DuLac, et al.,14 observed in a root canal system with lateral canals prepared in resin blocks that the carrier-based technique filled the cervical, middle, and apical third significantly better with gutta percha than lateral condensation. Wolcott, et al.,19 observed on resin models with simulated lateral canals that both techniques were equally effective in filling lateral canals, but there was significantly more gutta percha in the lateral canals with the gutta percha-coated rigid carrier technique. In contrast, the cold lateral condensation technique had significantly more sealer in the lateral canals. These findings were corroborated in the present study.
From a clinical point of view, it is important to highlight different authors’ statements that lateral canals may not be completely sealed even when radiographic images show a complete obturation. The penetration of the filling material in the lateral canal can give a false image.1,3,7,8 Therefore, in this study, the following categories were considered in the evaluation of radiographs: not obturated, partially obturated, and totally obturated. These radiographic results were confirmed with an analysis of the cleared specimens.
In relation to the caliber of the simulated lateral canals, these were drilled to a diameter of approximately 150 µm, corresponding to Engine Reamer No. 15. This caliber is related to what Kasahara, et al.,22 have observed in maxillary incisors and Miyashita, et al.,23 in mandibular incisors.
On the other hand, under in vivo conditions, organic debris that remains inside the lateral canals is difficult to remove through instrumentation and irrigation, and its presence can hinder the obturation of lateral and accessory canals. Hence, in this study, a paraffin gel was introduced inside the root canal previously instrumented and irrigated to simulate this situation Moreover, the roots of the specimens were covered with a thin foam rubber and Teflon to create a barrier to mimic the periodontal ligament.7,24,25
As Reader, et al.,18 and Goldberg, et al.,26 state, the accumulation of smear layer, produced during instrumentation, may block the entrance of the lateral canal. Due to this, EDTA 17% and EndoActivator were used in both samples to remove the smear layer. The removal of the smear layer with EDTA facilitates the obturation of lateral and accessory canals.26,27
Conclusion
Simulated lateral canals were frequently obturated by both techniques, but in those obturated with GuttaCore, a tendency to fill the lateral canals with gutta percha was observed.
Acknowledgments
Appreciation to Dr. Ricardo L. Macchi for his collaboration in the statistical evaluation.
After reading about this research on the single gutta-percha cone technique and GuttaCore, check out Dr. John West’s article, “Do lateral canals really matter?” here.
- Ricucci D, Loghin S, Siqueira JF Jr. Exuberant biofilm infection in a lateral canal as a cause of short-term endodontic treatment failure: report of a case. J Endod. 2013;39(5):712-718.
- De Deus QD. Frequency, location, and direction of lateral, secondary, and accessory canals. J Endod. 1975;1(11):361-366.
- Ricucci D, Siqueira JF Jr. Fate of tissue in lateral canals and apical ramifications in response to pathologic conditions and treatment procedures. J Endod. 2010,36(1):1-15.
- Schilder H. Filling root canals in three dimensions. Dent Clin North Am. 1967;11:723–744.
- Seltzer S. Endodontology — biologic considerations in endodontic procedures. New York, NY: McGraw-Hill; 1971.
- Weine F. The enigma of the lateral canal. Dent Clin North Am. 1984;28(4):833-852.
- Almeida JF, Gomes BP, Ferraz CC, Souza-Filho FJ, Zaia AA. Filling of artificial lateral canals and microleakage and flow of five endodontic sealers. Int Endod J. 2007;40(9):692-699.
- Venturini M, Di Lenarda R, Prati C, Breschi L. An in vitro model to investigate filling of lateral canals. J Endod. 2005;31(12):877-881.
- Gutmann J. Innovative changes in core-carrier root canal obturation. Endodontic Practice US. 2012;5(2):36-41.
- Canzani JH, Testa R, Garcia Fernandez E, Santía C. Transparencia de dientes. Su utilidad en la enseñanza preclínica de la endodoncia. [Tooth transparencies. Its use in the preclinical teaching of endodontics]. Rev Asoc Odontol Argent. 1984;72(3):72-73.
- Gordon MP, Love RM, Chandler NP. An evaluation of .06 tapered gutta-percha cones for filling of .06 taper prepared curved root canals. Int Endod J. 2005;38(2):87-96.
- Manfré S, Goldberg F. Evaluación del ajuste y adaptación de los conos de gutapercha ProTaper al conducto radicular instrumentado con el sistema ProTaper Universal. Endodoncia. 2010;28(3):135-140.
- Chesler MB, Tordik PA, Imamura GM, Goodell GG. Intramanufacturer diameter and taper variability of rotary instruments and their corresponding gutta-percha cones. J Endod. 2013;39(4):538-541.
- DuLac KA, Nielsen CJ, Tomazic TJ, Ferrillo PJ Jr, Hatton JF. Comparison of the obturation of lateral canals by six techniques. J Endod. 1999;25(5):376-380.
- Goldberg F, Artaza LP, De Silvio A. Effectiveness of different obturation techniques in the filling of simulated lateral canals. J Endod. 2001;27(5):362-364.
- Gurgel-Filho ED, Feitosa JP, Gomes BP, et al. Assessment of different gutta-percha brands during the filling of simulated lateral canals. Int Endod J. 2006;39(2):113-118.
- Karabucak B, Kim A, Chen V, Iqbal MK. The comparison of gutta-percha and Resilon penetration into lateral canals with different thermoplastic delivery systems. J Endod. 2008;34(7):847-849.
- Reader CM, Himel VT, Germain LP, Hoen MM. Effect of three obturation techniques on the filling of lateral canals and the main canal. J Endod. 1993;19(8):404-408.
- Wolcott J, Himel VT, Powell W, Penney J. Effect of two obturation techniques on the filling of lateral canals and main canal. J Endod. 1997;23(10):632-635.
- Goldberg F, Araujo JA. Estudio comparativo de la penetración de la gutapercha en las irregularidades del conducto radicular: sistema GuttaCore y técnica de cono único. [Comparative study of gutta-percha penetration in the root canal irregularities: GuttaCore system and single cone technique.] Rev Asoc Odontol Argent. 2016;104(1):4-8.
- Manzur E, Caplan V, Ballachino M, Goldberg F. Evaluación comparativa de la adaptación de la obturación endodóntica a las paredes del conducto radicular con dos técnicas de obturación. [Comparative evaluation of the adaptation of the endodontic obturation to the root canal walls with two filling techniques.] Rev Asoc Odontol Argent. 2016:104(3):95-101.
- Kasahara E, Yasuda E, Yamamoto A, Anzai M. Root canal system of maxillary central incisor. J Endod. 1990;16(4):158-161.
- Miyashita M, Kasahara E, Yasuda E, Yamamoto A, Sekizawa T. Root canal system of mandibular incisor. J Endod. 1997;23:479-484.
- Goldberg F, Artaza LP, Alfie D. Capacidad de diferentes procedimientos de irrigación para la remoción del barro dentinario del orificio pulpar de conductos laterales simulados. Rev Asoc Odontol Argent. 2010:98:113-118.
- de Gregorio C, Estevez R, Cisneros R, Paranjpe A, Cohenca. Efficacy of different irrigation and activation systems on the penetration of sodium hypochlorite into simulated lateral canals and up to working length: an in vitro study. J Endod. 2010;36(7):1216-1221.
- Goldberg F, Massone JE, Spielberg C. Effect of irrigation solutions on the filling of lateral root canals. Endod Dent Traumatol. 1986;2(2):65-66.
- Villegas JC, Yoshioka T, Kobashayi Ch, Suda H. Obturation of accessory canals after four different final irrigation regimes. J Endod. 2002;28(7):534-536.
Stay Relevant With Endodontic Practice US
Join our email list for CE courses and webinars, articles and more..
