Dr. Monika Dzieciątkowska presents a case demonstrating the reconstruction of a tooth with composite endocrown following an endodontic procedure
[userloggedin]

 This patient attended for root canal treatment and reconstruction of tooth LL6. According to the classic procedure, following root canal treatment, reconstruction includes a post and a crown. This, however, is associated with excessive hard tissue removal on the lingual and labial surfaces. (A composite restoration carried out on the distal surface prior to endodontic treatment was present on the distal surface.)
This patient attended for root canal treatment and reconstruction of tooth LL6. According to the classic procedure, following root canal treatment, reconstruction includes a post and a crown. This, however, is associated with excessive hard tissue removal on the lingual and labial surfaces. (A composite restoration carried out on the distal surface prior to endodontic treatment was present on the distal surface.)
Contemporary evidence supports this view; at the present time it is considered that durability of non-vital teeth decreases along with the loss of hard tissue — i.e., the greater the loss, the greater their susceptibility to breaking or fracturing. This is why reconstruction techniques, which allow for preserving the tooth’s hard tissues, are of great interest.
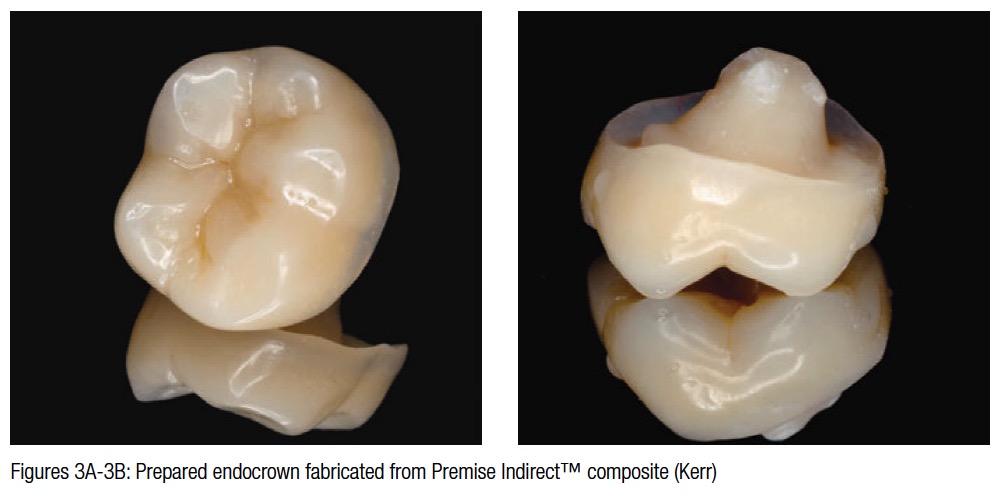
In this case, there exists a sufficient amount of hard tissue to justify producing an endocrown. An endocrown is an onlay made for a tooth undergoing endodontic treatment. The preserved lingual and palatal walls and the deep tooth chamber provided sufficient retention for such a prosthetic solution. An endocrown may be produced from composite or mineral ceramic, and because of the slightly lower cost and ease of repair of any potential damage, the patient chose the composite endocrown.
Preparation and treatment
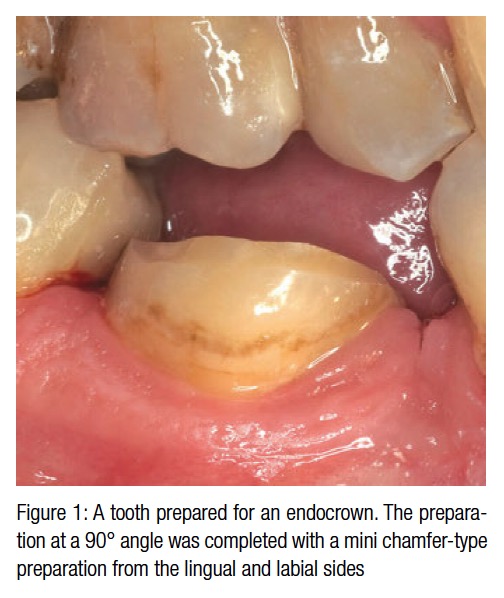
 The preparation at a 90° angle was completed with a mini chamfer-type preparation from the lingual and labial sides. Such a preparation is consistent with the prism course and ensures a good fusion of the bonding system with the enamel. All the sharp edges are smoothed out. The preparation was completed using a 40-micron diamond drill.
The preparation at a 90° angle was completed with a mini chamfer-type preparation from the lingual and labial sides. Such a preparation is consistent with the prism course and ensures a good fusion of the bonding system with the enamel. All the sharp edges are smoothed out. The preparation was completed using a 40-micron diamond drill.
A photograph with a shade guide (one or two basic shades were chosen) and an impression made with a polyvinyl siloxane (or polyether) material were sent to the laboratory.
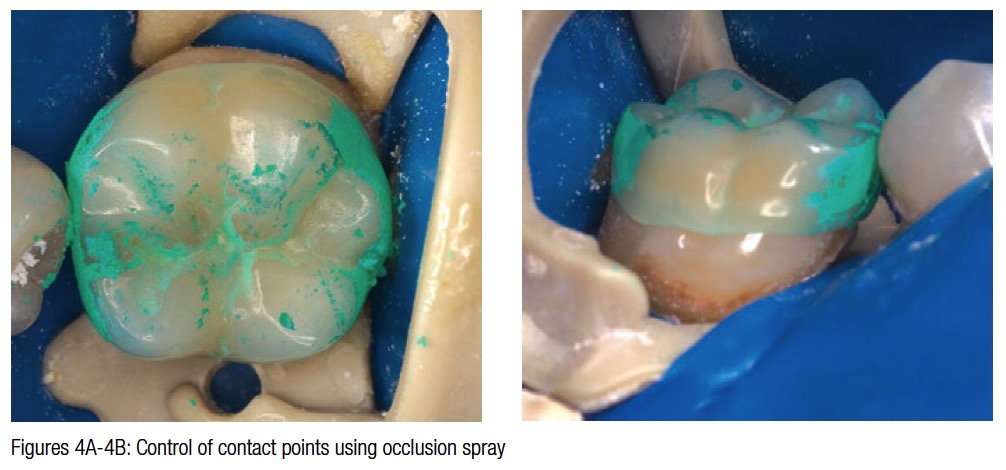
The next appointment involved implementation of the cementation procedure. A rubber dam (Optidam™ [Kerr] and a universal SoftClamp clamp [Kerr]) are indispensable for adhesive procedures. It is placed on the tooth to be reconstructed and the neighboring teeth, making it possible to control the contact point. Careful control of a close fit to adjoining teeth is very important. In this case, contact points were too tight, and the onlay would not stay in place. In order to find and control contact points in the mouth, occlusion spray is used. Thus, the areas that may hinder the procedure are eliminated.
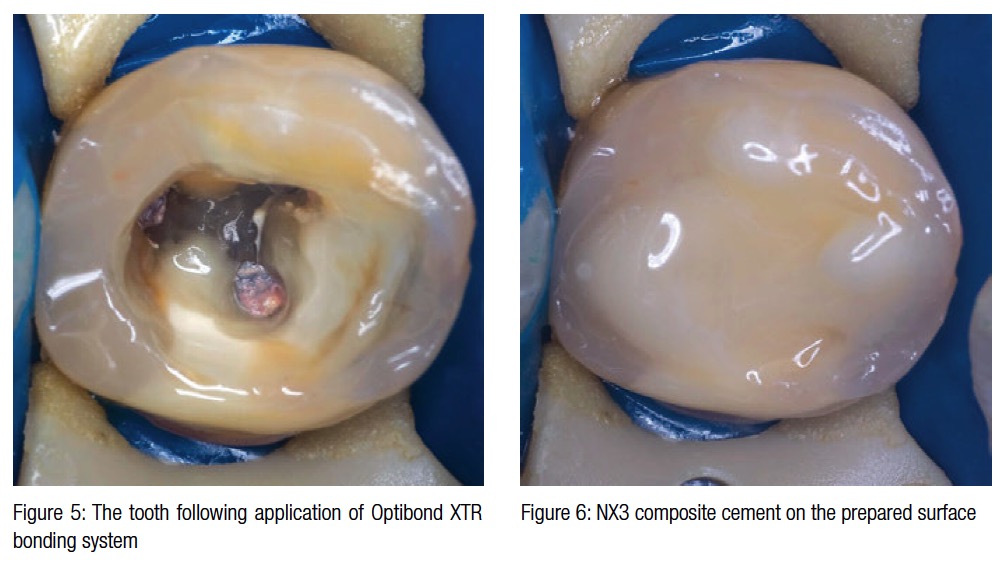
To embed the endocrown, a sixth-generation self-etch bonding system (Optibond® XTR [Kerr]) was used, which was spread on the surface of the preparation and then light-cured. A dual-cured composite resin cement (NX3) was also spread on the surface of the preparation.
Results
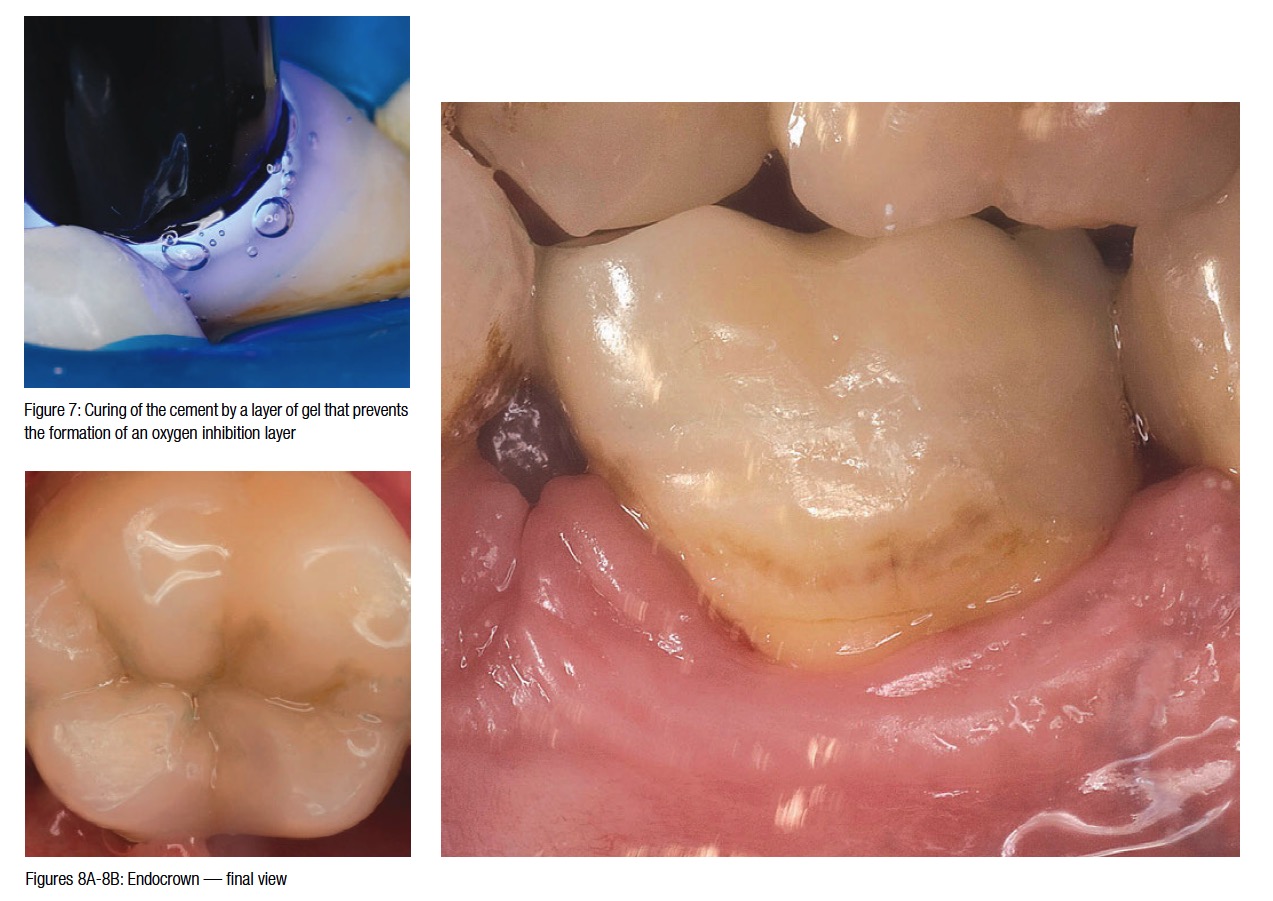
Following the mounting procedure and the initial removal of any excess, the cement was polymerized. The initial short polymerization was completed by a long polymerization (40 seconds for each surface) using a gel that stopped the creation of an oxygen-inhibition layer. This ensured that the material would not change color or dissolve. This type of dual-cured composite resin cement (NX3) was indispensable because of the thickness of the endocrown and the difficulties associated with light from the curing unit penetrating into the deepest spaces.
[/userloggedin]
[userloggedout][/userloggedout]
Stay Relevant With Endodontic Practice US
Join our email list for CE courses and webinars, articles and more..
