Dr. Godfrey Cutts discusses repair of a perforation of the floor of the pulp chamber with Biodentine®
Case study
A 43-year-old female patient was referred for possible endodontic treatment to the UL6 by her dental practitioner who stated in the referral letter that there was a possible perforation of the floor of the pulp chamber, which had been “temporized with amalgam”
[userloggedin]
(Figure 1). 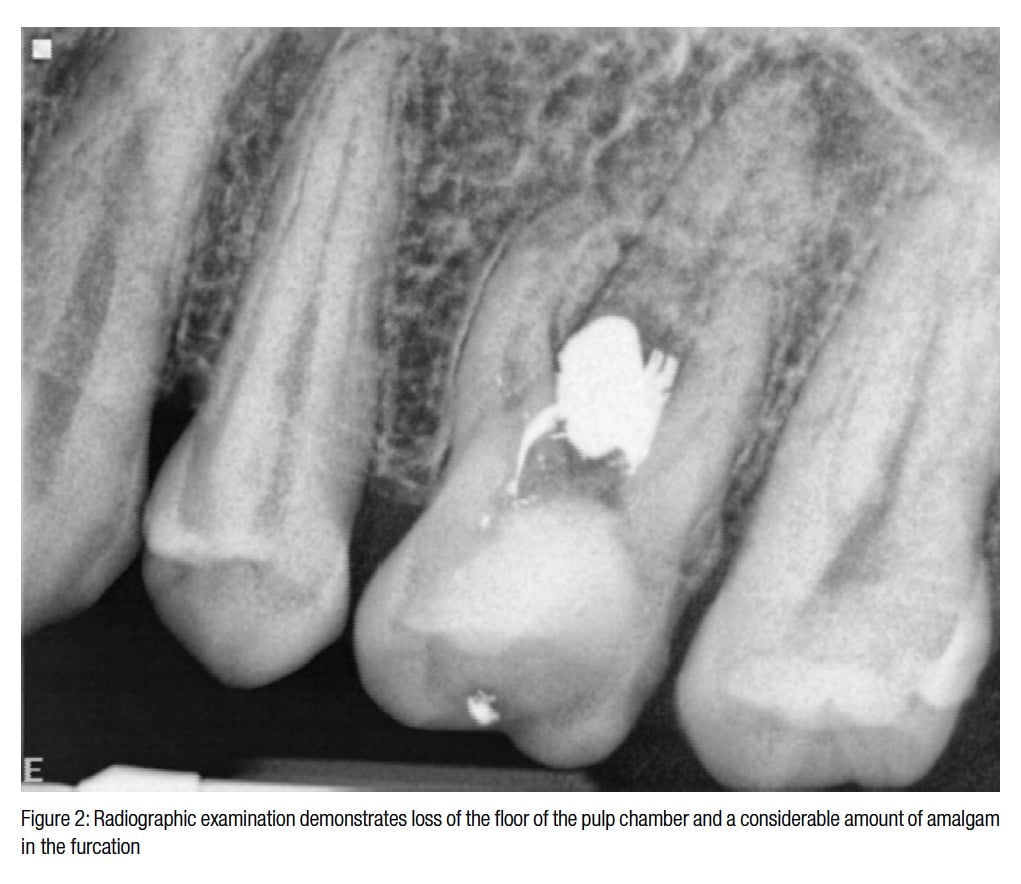 Upon examination, there was some buccal tenderness, and the tooth was slightly tender to percussion. Radiographic examination showed loss of the floor of the pulp chamber and a considerable amount of amalgam in the furcation (Figure 2).
Upon examination, there was some buccal tenderness, and the tooth was slightly tender to percussion. Radiographic examination showed loss of the floor of the pulp chamber and a considerable amount of amalgam in the furcation (Figure 2).
Local anesthetic was administered and the tooth isolated with rubber dam. After removal of the coronal temporary dressing, the extent of the perforation was revealed. It involved the whole of the floor of the pulp chamber, including the orifice of the palatal and distobuccal canals (Figure 3).
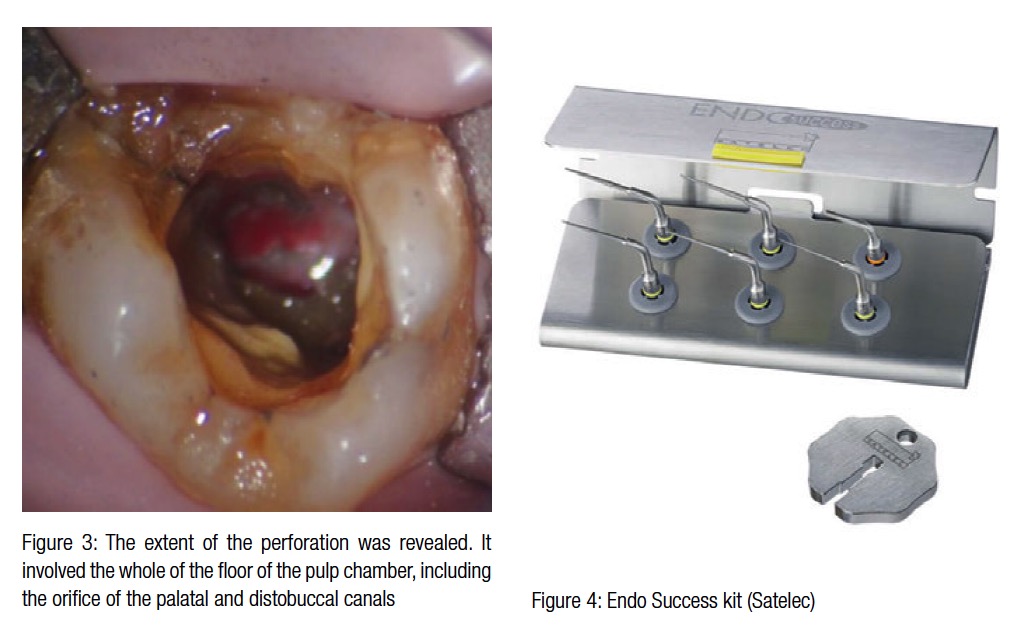 The amalgam could not be removed intact since it was convex and locked in the furcation. With judicious use of ultrasonic instruments from the Satelec® Endo Success™ range (Figure 4), the amalgam was gently fragmented and the majority removed.
The amalgam could not be removed intact since it was convex and locked in the furcation. With judicious use of ultrasonic instruments from the Satelec® Endo Success™ range (Figure 4), the amalgam was gently fragmented and the majority removed.
A change of plan
 The initial treatment plan was to carry out conventional endodontic treatment before repairing the perforation; however, this was not possible since the irrigants were leaking through the furcation and past the rubber dam. Repair of the perforation became the priority, and this was carried out using Biodentine® (Septodont).
The initial treatment plan was to carry out conventional endodontic treatment before repairing the perforation; however, this was not possible since the irrigants were leaking through the furcation and past the rubber dam. Repair of the perforation became the priority, and this was carried out using Biodentine® (Septodont).
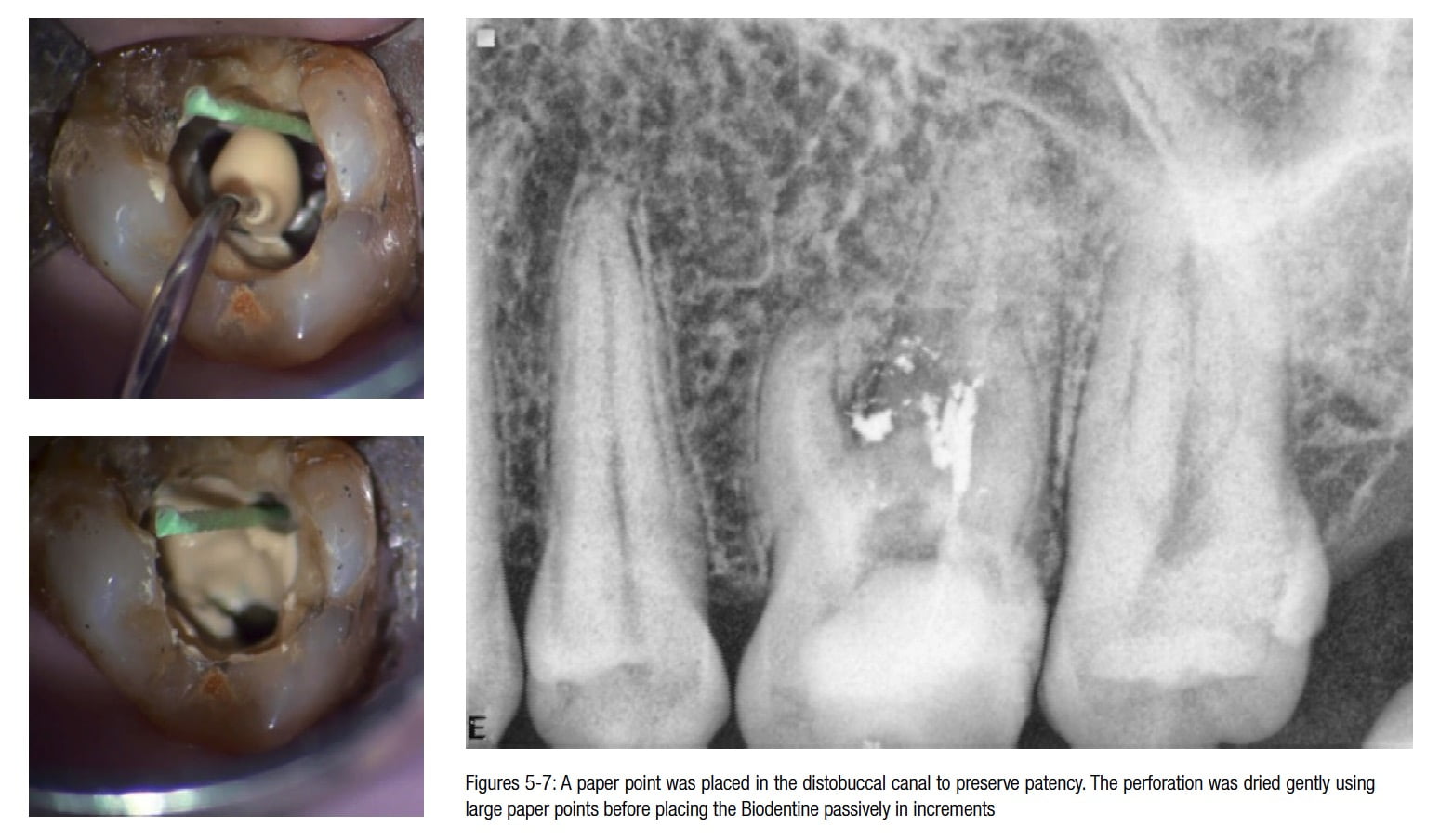
Before attempting the repair, a paper point was placed in the distobuccal canal to preserve patency. The perforation was dried gently using large paper points before placing the Biodentine passively in increments using a Thymozin instrument (Figures 5-7). Upon completion of repair of the perforation, the Biodentine was allowed to set for 10 minutes before temporization of the access cavity.
Second visit
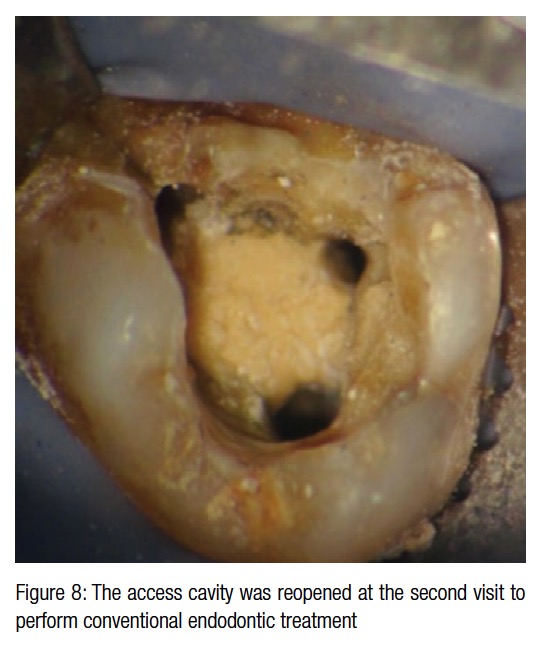
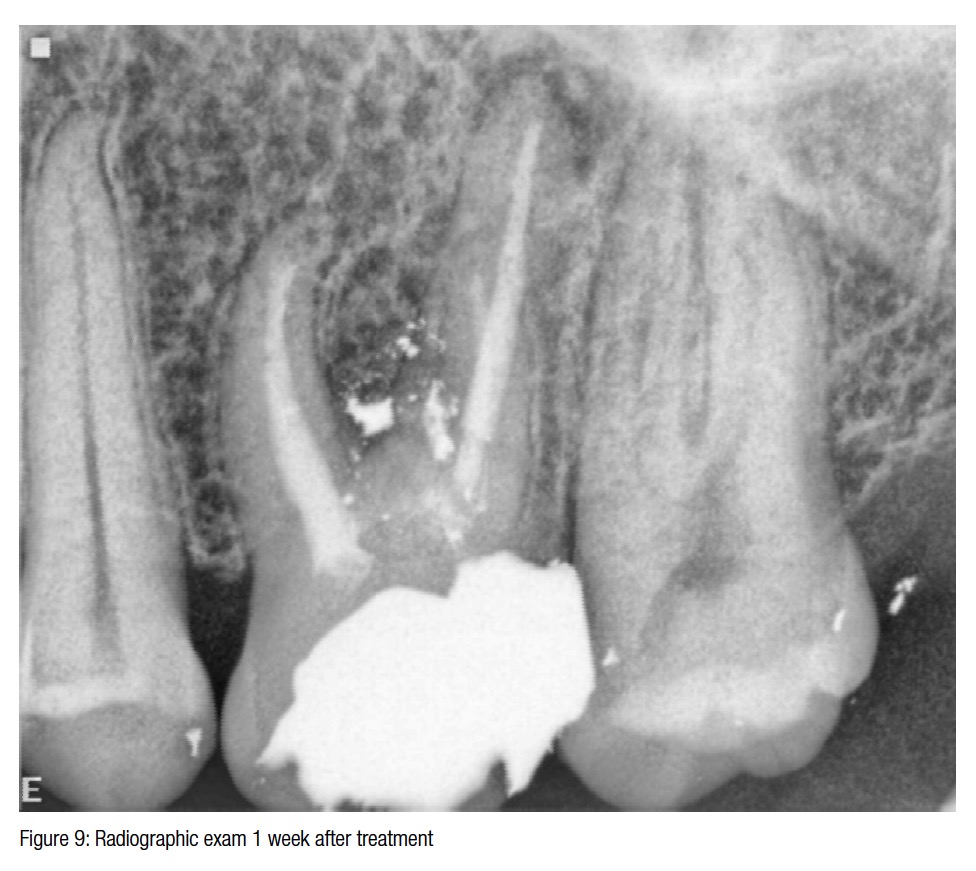 At the second visit, 1 week later, the access cavity was reopened (Figure 8) to perform conventional endodontic treatment with glass ionomer cement used to restore the floor of the access cavity followed by a bonded amalgam core (Figure 9). The tooth was removed from the occlusion, and the patient was advised to have a full coverage crown as soon as possible.
At the second visit, 1 week later, the access cavity was reopened (Figure 8) to perform conventional endodontic treatment with glass ionomer cement used to restore the floor of the access cavity followed by a bonded amalgam core (Figure 9). The tooth was removed from the occlusion, and the patient was advised to have a full coverage crown as soon as possible.
[/userloggedin]
[userloggedout][/userloggedout]
Stay Relevant With Endodontic Practice US
Join our email list for CE courses and webinars, articles and more..
