Dr. Reid Pullen discusses ProTaper Ultimate and other systems that can lead to effective, efficient treatment.
Dr. Reid V. Pullen uses a safe, effective, and efficient shaping system to paint a “beautiful endodontic canvas”
Endodontic treatment often starts with two questions: (1) Can we shape the canal system safely, effectively, and efficiently? (2) Can we do this in a minimally invasive manner, preserving precious tooth structure while eliminating necrotic tissue and microbes to produce a healing environment?
With the advent of enhanced disinfection — GentleWave® (Sonendo®), SWEEPS® (Shock Wave-Enhanced Emission Photoacoustic Streaming, Fotona), the SmartLite® Pro EndoActivator® (sonic activation, Dentsply Sirona), EndoUltra® (ultrasonic activation, Vista), EndoVac™ (apical negative pressure system, Kerr Dental), and the Gentlefile® Smart System (Tornado Disinfection Kit, Medic NRG) — the hope is that endodontic therapy can be performed in a minimally invasive manner, while maximally disinfecting the canal system (Figures 1, 2, and 3).

Two of these devices, GentleWave (Figure 4) and SWEEPS (Figure 5) have generated interest in the field of endodontics and show potential at effectively debriding a minimally shaped canal system verses standard needle irrigation (SNI). GentleWave, with the new CleanFlow® procedure instrument, emits multisonic sound waves in the presence of degassed sodium hypochlorite and EDTA. This device is able to remove the majority of pulp tissue and microbes from the root canal system in minimally shaped canals.1 SWEEPS emits a photon laser pulse pair into sodium hypochlorite and EDTA, which creates a hypersonic shockwave in the canal.2 Both systems have shown to be effective at removing canal debris and microbes.1,3

Chemical debridement is only one piece of the endodontic minimally invasive puzzle. At this point in time, we must shape the canals in order to provide space for obturation materials. There are many file systems on the market that are able to safely shape canals in a minimally invasive protocol. TruNatomy™ (Dentsply Sirona) (Figure 6) is one file system that preserves pericervical dentin, which can be critical in the long-term success of tooth retention.4 DCTaper™ (formerly VTaper) (SS White) is another popular file system that minimally shapes canals and preserves coronal dentin.5

A recently released file system called ProTaper Ultimate™ (Dentsply Sirona) (Figure 7) may change the way we perform endodontic therapy. ProTaper Ultimate was designed and created by Drs. Cliff Ruddle, John West, and Pierre Machtou. The new objective of this file system is to take the design and enhanced metallurgy from ProTaper Gold™ and produce a file system that safely shapes effectively, efficiently, and minimally. This article will discuss the new minimally invasive endodontic shaping system, ProTaper Ultimate, and discuss why it is a novel shaping system.
ProTaper Ultimate starts with a whole new mindset — a mindset unfamiliar with most clinicians. The universal mindset that states, “Always explore and ‘secure’ the canal prior to introducing any nickel titanium shaping file,” has shifted to a new paradigm. This paradigm states that once the canals are located, move directly to the ProTaper Ultimate Slider. The Slider is a nickel-titanium file with a 0.16 tip, progressive taper made of M-Wire. In the majority of “simple to medium difficult” canal systems, it will negotiate down to estimated working length and, at the very same time, shape and cut an open glide path to aid in subsequent file usage. This is revolutionary in the fact that the canal is not first secured by a hand file, and that a coronal flare is not always necessary. In the more difficult cases, whether it is an access issue or a constricted, calcified canal system, the auxiliary SX should be used to open up the coronal third and remove the dentinal cervical triangle.
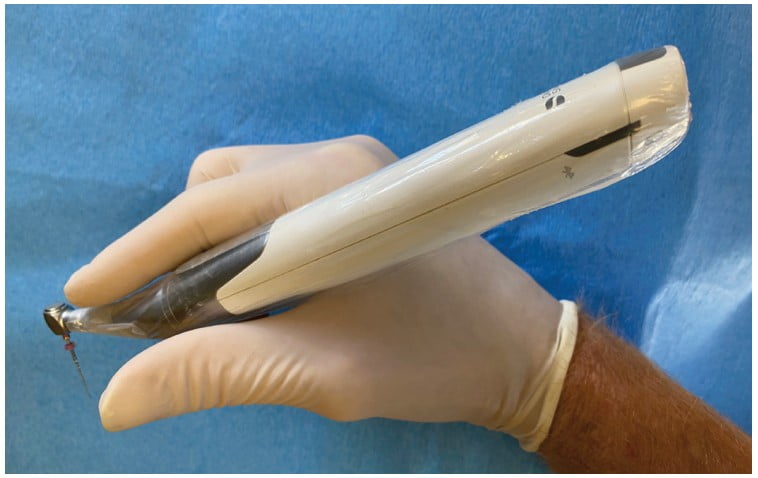
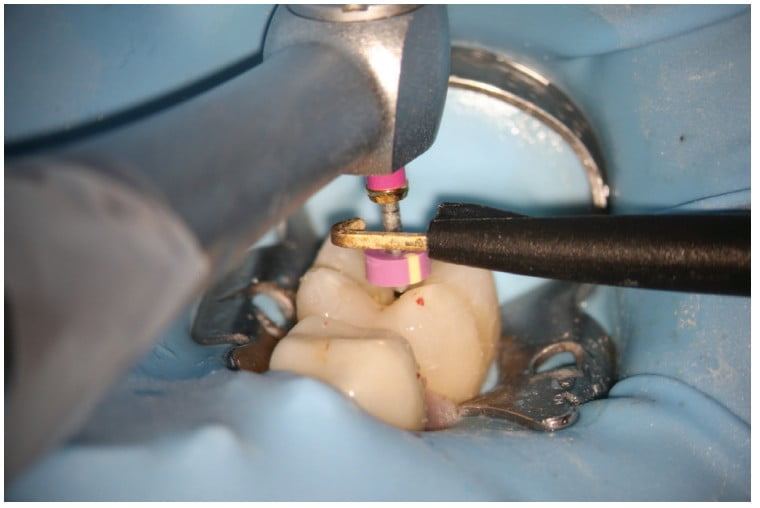
The Slider runs at 400 RPMs and at 5.0 Ncm torque. It is recommended to hold the handpiece in the webbing of your hand and to let it slide down the canal (Figure 8). It is estimated that about 65% of the time, the Slider will advance down to estimated working length (in the author’s experience it is more 80% to 90% of the time in simple cases) in 1-3 passes. At this point, either attach an Electronic Apex Locator (EAL) clip to the handle of the Slider (Figure 9) and obtain an accurate working length, or remove it and attain a working length with a No.10 hand file. Either way, the goal of the Slider is to effectively and efficiently slide down the canal to working length, open the canal, and create a glide path. If these three pillars of endodontic treatment (negotiation to patency, accurate working length, and open glide path) can be accomplished safely in 30 to 60 seconds and without the need of a hand file, the treatment time and difficulty can be reduced. Less treatment time, with less shaping and with enhanced disinfection, could lead to a decrease in adverse treatment events (file separation, ledging, etc.) and a more efficient procedure.
In the event of an apical curve or a constricted canal, and the Slider will not advance down to estimated working length, then remove it, and achieve negotiation and working length the traditional way, with hand files. The rule with the ProTaper Ultimate Slider is “restraint.” We must treat the canals as a painter treats a canvas — with elegant, gentle, deliberate brushstrokes. We are not construction workers hammering files into the canal. The key to this system is the Slider negotiating to patency, achieving an accurate working length, and creating an open glide path. If this is done using gentle brushstrokes, then the rest of the painting (shaping) of the canals can be effortless. The technique is as follows: employ 4-5 engagement/disengagements (gentle in-and-outs), and if the Slider has not advanced to the estimated working length, remove it, irrigate with sodium hypochlorite, and then continue with Pass No. 2. If the Slider will not advance, and it feels like it is hitting a “brick wall,” then remove it and negotiate to working length with a No. 10 hand file. Once working length is achieved, run the Slider to the end (working length), and achieve an open glide path. Now we are off to the shaping races. It is time to finish painting the canvas and creating a beautiful endodontic minimally invasive work of art. The canal is now secure and is just waiting to be cleaned and shaped.

The next step in the ProTaper Ultimate series is to use the Shaper. This is newly designed to reduce the shaping load by taking the ProTaper Gold S1 and S2 and combining it into one “super” Shaper. The shaper has a maximum file diameter of 1 mm verses the traditional 1.2 mm, aiding in conservation of cervical tooth structure, and it has a parallelogram cross section with a 0.20 tip. Typically, once the Slider advances to working length, the Shaper will also advance to the same area within one to two passes. The Shaper’s main job is to shape the coronal two-thirds of the canal system. Employ the same gentle shaping technique of 4-5 engagement/disengagements (pass No. 1). Then remove the Shaper, irrigate to remove the debris created during instrumentation with sodium hypochlorite, recapitulate, and move onto pass No. 2 until the Shaper reaches working length.
Now complete the final shape with the ProTaper Ultimate Finisher 1 (F1- #20 tip size). The F1 will easily advance to working length (or just short of it) once the Slider and Shaper have cut the path down to or close to working length. These are your finishing brushstrokes on the endodontic canvas.
At this point, as clinicians we must make a decision. For GentleWave or SWEEPS laser users, it is recommended to stop at F1 and 1 mm back from working length. The final touches or brush-ups on the endodontic canvas are achieved by using these enhanced disinfection protocols. If you do not use either of these devices, then examine the F1 apical flutes. Are they full of dentinal shavings? Did the F1 create deep apical shape? If so, then the apical shape is complete. If the apical flutes are relatively free of debris, then advance to the ProTaper Ultimate F2. In the majority of non-large canals, the clinician will finish with the F2. (In the author’s experience, if not using enhanced disinfection devices then the canals are usually finished with the F2.) In some larger canals, the ends of the apical flutes of the F2 will also be free of debris, and you will need to advance to the F3 (No. 30 tip size) or the FX (No.35 tip) or the FXL (No. 50 tip).
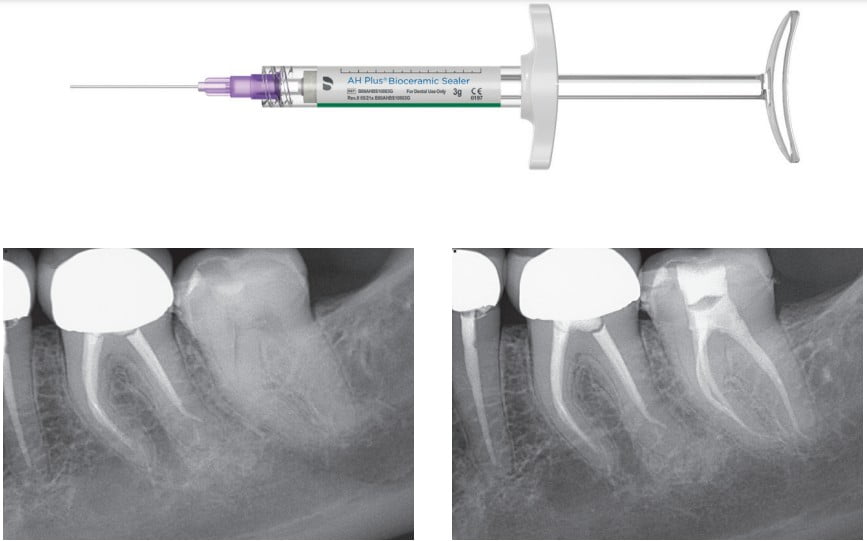
Once shaping is complete, perform apical verification with the corresponding hand file, irrigate, recapitulate, and place matching ProTaper Ultimate gutta-percha cones to working length. These new cones are flat ended, have an extended heat wave, and are precision-machined to fit the shape that was prepared. Once the cone-fit radiographs are completed, and if not using SWEEPS or GentleWave, then use of the sonically driven EndoActivator to enhance disinfection is utilized. (Figure 10). The new EndoActivator (sonic activation) is improved with increased cycles per minute, an elliptical movement pattern, and a newly designed polymer tip that acts as a paddle with fins. The MIE canvas is created by the dual brushstrokes of shaping and enhanced disinfection. Disinfection and cleaning of the root canal system entails removing necrotic tissue, biofilms, microbes, and the smear layer created by shaping. Once the smear layer is removed, single cone obturation can be used with the new AH-Plus® Bioceramic Sealer (Dentsply Sirona) (Figure 11). The bioceramic sealer has high radiopacity and demonstrates good anatomical fill of the prepared canal system (Figures 12 and 13). This sealer has greatly improved properties of traditional bioceramic sealers with an overall 4-hour set time and a 0.11% solubility rating (internal study, Dentsply Sirona).
If you have had mixed results using bioceramic sealers, then complete the endodontic painting with your obturation of choice. I prefer warm vertical obturation using either Pulp Canal Sealer™ EWT (zinc oxide eugenol, Kerr Dental) or Ribbon® Root Canal Sealer (epoxy-resin, Dentsply Sirona). I prefer the black Gutta-Smart™ (Dentsply Sirona) heat tip (40/.025) to remove the coronal two-thirds gutta percha and the Dovgan Pluggers to gently push and form the gutta-percha apical plug into the foramen. I then use the 25 gauge tip on the backfill of the cordless Gutta-Smart with a pen grasp and backfill the canals one after the other in a very efficient manner.
The ProTaper Ultimate file system is a new approach that represents a shift in the shaping paradigm. It is now recommended to start with a rotary, nickel-titanium shaping file (Slider) prior to securing the canal with hand files. This system, like others, comes with matching paper points, gutta-percha cones, and with gutta-percha obturators being introduced soon. In the end, the ultimate goal is to provide the clinician with a safe, effective, and efficient shaping system that can paint a beautiful endodontic canvas without under-mining sound tooth structure.
Read more about ProTaper Ultimate in “The new Endo Solution: Performance Unlimited with ProTaper Ultimate” at https://endopracticeus.com/industry-news/the-new-endo-solution-performance-unlimited-with-protaper-ultimate/
 Reid V. Pullen, DDS, graduated from USC Dental School in 1999. He completed an advanced education in general dentistry in 2000 while serving in the Army Dental Corps in Landstuhl, Germany. He graduated from the Long Beach VA Endodontic Residency in 2006 and opened a private practice in Brea, California, in 2007. Dr. Pullen became a Diplomate of the American Board of Endodontics in 2013.
Reid V. Pullen, DDS, graduated from USC Dental School in 1999. He completed an advanced education in general dentistry in 2000 while serving in the Army Dental Corps in Landstuhl, Germany. He graduated from the Long Beach VA Endodontic Residency in 2006 and opened a private practice in Brea, California, in 2007. Dr. Pullen became a Diplomate of the American Board of Endodontics in 2013.
Disclosure: Dr. Pullen is a speaker for Dentsply Sirona.
- Vandrangi P, Basrani B. Multisonic Ultracleaning in Molars with the GentleWave® Oral Health. 2015;72-86.
- Yang Q, Liu MW, Zhu LX. Micro-CT study on the removal of accumulated hard-tissue debris from the root canal system of mandibular molars when using a novel laser-activated irrigation approach. Int Endod J. 2019;53(4):529-538.
- Molina B, Glickman G, Vandrangi P, Khakpour M. Evaluation of Root Canal Debridement of Human Molars using the GentleWave System. J Endod. 2015;10:1701-1705.
- Kumar M, Paliwal A, Manish K, et al. Comparison of Canal Transportation in TruNatomy, ProTaper Gold, and Hyflex Electric Discharge Machining File Using cone-Beam Computed Tomography. J Contemp Dent Pract. 2021;22(2):117–121.
- Shenoi, P, Luniya, D, Badole, G, et al. Comparative evaluation of shaping ability of V-Taper 2H, ProTaper Next, and HyFlex CM in curved canals using cone-beam computed tomography: An in vitro study. Indian J Dent Res. 2017;28:181-186.
Stay Relevant With Endodontic Practice US
Join our email list for CE courses and webinars, articles and more..
