Oehlers Type IIIB dens invaginatus can be treated with correct planning, thorough cleaning of the internal anatomy, and adequate three-dimensional obturation.
Drs. Gonzalo García, Claudia Judkin, Denise Alfie, Ariel Lenarduzzi, and Pablo Alejandro Rodríguez discuss treatment of a complex dental anomaly
Abstract
The complex anatomy of an Oehlers Class IIIB dens invaginatus (DI) in a maxillary lateral incisor is a major endodontic challenge for the endodontist.
Method
The case reported here is a 14-year-old male patient referred for clinical evaluation with a fistula associated with the maxillary lateral incisor. The crown had no signs of alteration, just slightly wider mesiodistally compared to its contralateral. Pulp testing showed negative results. The images obtained revealed an extensive apical radiolucency. The diagnosis was pulp necrosis with a periapical lesion in an upper lateral incisor with an image coincident with DI.
Results
In this case, the endodontic treatment of the root canal system was performed in three sessions. Irrigation with 2.5% sodium hypochlorite plus the use of an activating device played a very important role in cleaning the DI. The endodontic obturation was performed with a dual thermoplastic gutta-percha system to obtain an adequate three-dimensional filling. The 3-year recall showed complete healing of the periapical tissues.
Conclusion
Endodontic success in these cases can be achieved through correct planning, thorough cleaning of the internal anatomy, and adequate three-dimensional obturation.
Introduction
Among dental malformations, dens invaginatus (DI) is one of the most frequent. This development anomaly arises from the invagination of the internal epithelium of the enamel organ within the dental papilla before the calcification of the tissues. Affected teeth may present, in the crown and/or roots, variations in shape and size.1 Radiographically, this presents an invagination of the enamel and dentin that can reach the pulp chamber, the root, and in some cases, even the apex. This alteration is usually asymptomatic and in many cases, its detection is a random radiographic finding.
DI was first described in 1856 by a dentist called Socrates.2 Mühlreither in 1873 reported … “anomalous cavities in human teeth.” Baume in 1874 and Busch in 1897 also published this malformation.3-5 In 1897, Tomas describes DI in his textbook, A System of Dental Surgery.1-3
DI can occur in any dental group and in temporary or permanent teeth; however, it occurs more frequently in the upper lateral incisor. Forty-two percent of reported cases are linked to that tooth. Its incidence in the population ranges from 0.04% to 10%,6 being more frequent in men.7 Probably the percentages observed in the literature are so variable because the studies were conducted in different population groups, and the diagnostic criteria used were not equal.8
Various treatment modalities have been proposed to address the pathologies associated with DI. These procedures range from prophylactic restorations to endodontic treatments, complementary surgery, or even extraction.9-11 Undoubtedly, the clinical resolution of a DI, which requires nonsurgical endodontic treatment, represents a great challenge for the specialist.
Classification of dens invaginatus
Different classifications have been suggested to describe DI. The first was published by Hallet in 1953.14 However, one classification of Oehlers, proposed in 1957, is the most used.12-13 This author divided the DI into three categories according to the depth of penetration and communication with the periapical tissues and the periodontal ligament.
Type I: The invagination is small, communicates with the enamel, is limited to the crown of the tooth, and does not exceed the level of the cementoenamel junction.
Type II: The invaginated depth of the enamel reaches the root, remaining hidden inside it. It may or may not have communication with the pulp tissue, but it does not have it with the periodontal ligament.
Type IIIA: The invagination penetrates through the root and communicates apically or laterally in the foramen, sometimes refers to a second foramen in the root. Normally, there is no communication with the pulp.
Type IIIB: The invagination extends through the root and communicates with the periodontal ligament in the apical foramen. Normally, it has no communication with the pulp.
Case report
A 14-year-old male was seen at dental school of the University of Buenos Aires in December 2015, referred by the orthodontic specialist. Clinical examination revealed the presence of a sinus tract at the level of the right upper lateral incisor. The crown of the tooth was complete, and it was slightly wider than the crown of the contralateral tooth. On the periodontal examination, no abnormal depth pockets were found. A panoramic radiograph shows unusual dental anatomy and a radiolucency image surrounding the apex.
To determine the origin of the sinus tract, a gutta-percha cone was placed along its path, and a periapical radiograph was taken. The image obtained confirmed that the tooth No. 1.2 was the cause of the infection and allowed to visualize the presence of a distal root canal of normal configuration and a larger pulp space toward the mesial. (Figures 1A and 1B, Figure 2)

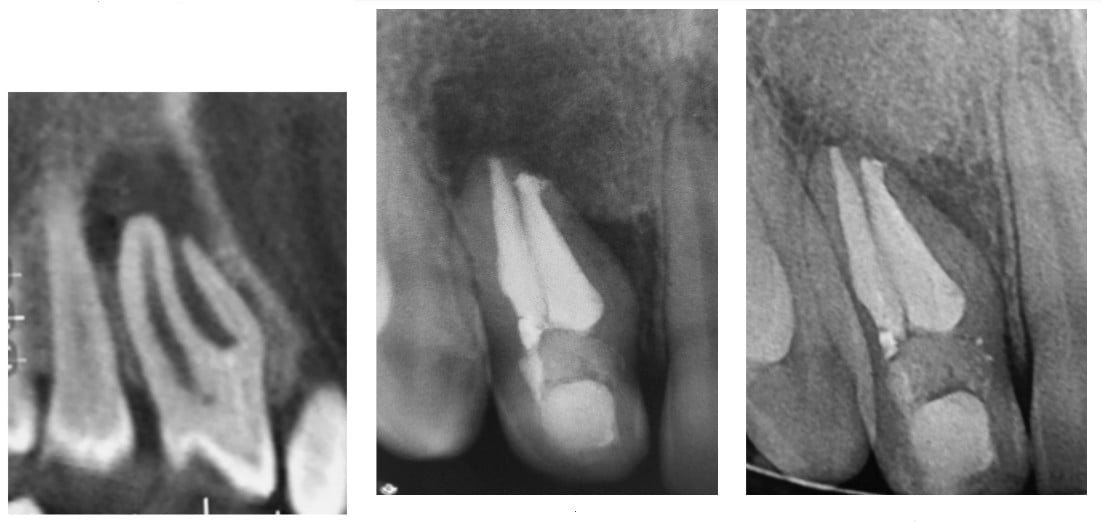
A cone beam computed tomographic imaging (CBCT) was captured for a more precise diagnosis. The images obtained confirmed the presence of an Oehlers Class IIIB DI (Figure 3). Informed consent was obtained from the parents to carry out the treatment, and at the first appointment, conventional access was performed under local infiltrative anesthesia (Totalcaina Forte; Laboratorios Bernabo, Buenos Aires, Argentina) and rubber dam isolation.
After the access, the distal canal was negotiated, and purulent drainage occurred spontaneously. An electronic apical locator (Root ZX®; J Morita Corp.) was used to determine the working length and confirmed radiographically.
The main canal was cleaned and shaped with K-files (Dentsply Sirona) with a step-back technique up to a No. 50 apically and irrigated with 2.5% of sodium hypo-chlorite. After the use of paper points, calcium hydroxide mixed with distilled water was used as intracanal dressing and a temporary sealing with Ionofil Molar glass ionomer (VOCO, Cuxhaven, Germany) was placed on the access cavity.
In a second appointment, 15 days later, clinical examination revealed that the sinus tract had disappeared, and the final obturation of the main canal was performed with lateral compaction technique of gutta-percha points (Meta-Biomed, Korea) and AH Plus® sealer (Dentsply Sirona) In the same appointment, the DI was located using an operative microscope (OPMI pico, ZEISS).
Profuse drainage of pus occurred again during the access. The working length was verified through the use of an apex locator and a periapical radiographic image; 2.5% sodium hypochlorite was used as irrigation and activated with EndoActivator® (Dentsply Sirona). At the end of this appointment, an intracanal dressing based on calcium hydroxide and a temporary sealing with Ionofil Molar were placed.
In a third appointment, the calcium hydroxide dressing was removed with copious irrigation, and the removal was completed with the XP endo-Finisher file (FKG Dentaire SA, La Chaux-de-Fonds, Switzerland). The apical gauge of the DI was confirmed with a No. 60 K-file. Finally, irrigation was carried out with 2.5% sodium hypochlorite for 5 minutes and dried with paper points.
The final obturation of the DI was done by thirds using a thermoplastic gutta-percha system. The Calamus® Dual system (Dentsply-Sirona) was used for this purpose in the apical third using the continuous wave of obturation technique after adjusting a No. 60 gutta-percha point. The remaining canal was back-packed with the Calamus Flow handpiece (Figure 4).The sealer used was AH Plus. The access was restored with Ionofil Molar.
Clinical and radiographic controls were performed initially every 3 months and, after the second recalls, every 6 months until the complete reparation of the periapical tissues was confirmed. Periapical radiography (Figure 5) and CBCT were performed in the 3-year recall. Both images showed complete apical healing, and the patient was asymptomatic.
Discussion
DI is always a challenging case for endodontic treatment since such teeth always have a complex root canal morphology.1-14 Various treatment options have been reported in the literature including preventive restorations, endodontic treatment, a combination of endodontics and surgery, intentional reimplantation, or extraction. The decision to choose one of them is related to the type and extent of the invagination.10,15,16 The clinical case treated in this article was Oehlers Class III Type B DI in a superior lateral incisor with periapical lesion.12
An accurate radiographic examination is necessary for the detection of the DI. However, periapical radiographs and/or panoramic images may not reveal details of the type and extent of invagination.17,18 Texeiro, et al., noted that the use of CBCT has become a very valuable tool, not only for diagnosis, but also for planning and treatment. Nonetheless, its use requires higher doses of radiation, so its indication must be precise and applied correctly in each patient.19,20 The images obtained in this case allowed the analysis of the internal morphology, and confirmed the existence of independent foramen at the apex and the size of the invagination and the peri-radicular lesion.
These anomalies have a high incidence of infection and pulp degeneration, which is why its early detection is very important to establish preventive behaviors and avoid pulp necrosis and periapical inflammation.13 Not detecting and not treating these malformations can promote pulpal alterations in a short time after dental eruption even when the apex is not yet developed.21-23
In the present case at the first appointment, a sinus tract was detected clinically. The crown did not show alterations due to caries or pre-existing restorations. However, the literature mentions that the pathology can develop due to the presence of communicating canals between the invagination and the root space. This communication would occur because the enamel coating is incomplete.24,25
When a Type III DI is accompanied by an apical lesion, the indicated treatment in the first instance is conventional endodontic treatment. Its therapeutic management can be difficult due to the internal configuration of the root canal system, which makes cleaning and shaping arduous beyond the use of manual or mechanized techniques.7
Endodontic instruments are designed to clean and shape the dentin, but it is impossible to remove the enamel with them. In cases of Type III DI where the invagination is partially or completely covered with adamantine tissue, the conventional instrumentation will not be effective.26-27
On the other hand, the volume and shape of the DI make it very difficult for the instruments to reach the dentin surface. In this case, irrigation solutions and their activating systems play a very important role due to their ability to clean and disinfect the cavity.
The use of intermediate medication in endodontic treatment is a matter of debate in the literature because of the difficulties for its removal. Undoubtedly, this situation is even more complex in DI cases because of the presence of a large, irregular, and retentive cavity. In this case, when the access was performed in the DI, drainage occurred that required the placement of an intracanal dressing based on calcium hydroxide.
Several publications have reported success rates in removing calcium hydroxide with various techniques and devices such as sonic, ultrasonic irrigation, or even negative pressure systems (PUI).28-31 In this case, a sonic device, the EndoActivator, was used to activate sodium hypochlorite, and XP endo-Finisher was used to remove the intermediate medication. Due to its design and kinematics, XP endo-Finisher allows a larger internal surface of the root canal to be addressed, achieving better contact with the dentin wall.32 The combination of both systems made it possible to achieve a more efficient cleaning and removal of the intermediate medication.
Finally, achieving a three-dimensional seal becomes the last therapeutic challenge. In general, such wide-rooted spaces require the use of techniques that involve hot gutta percha even with the risk of overfilling. Injection systems are usually those of choice.33
In this case, a combined obturation technique was performed. Cold lateral condensation was used in the distal canal. In the DI, the Calamus Dual System, which combines two hot gutta-percha techniques, was used. The apical third was obturated with the continuous wave technique after achieving a correct fit of No. 60 gutta-percha cone and the middle and coronal thirds with the injection technique.
Conclusion
The treatment of a Type III DI is a big challenge for the specialist. Nonsurgical endodontic treatment is always considered as the first choice, no matter the size of the apical lesion.
Read about conservative treatment of a case of Oehlers Type IIIB dens invaginatus here: https://endopracticeus.com/ce-articles/nonsurgical-endodontic-treatment-of-a-maxillary-central-incisor-diagnosed-with-infected-dens-invaginatus-oehlers-type-iii-and-apical-periodontitis/
- Hülsmann M. Dens invaginatus: etiology, classification, prevalence, diagnosis, and treatment considerations. Int Endod J. 1997;30:79-90.
- Schulze C, Gorlin RJ, Goldman HM. Thomas Oral Pathology.6th ed. Vol. 1. St. Louis: CV Mosby; 1970. Developmental abnormalities of the teeth and jaws.
- Tomes J. A System of Dental Surgery. 3rd ed. London, UK: J.& A. Churchill.
- Oehlers F. Dens Invaginatus (dilated composite odontome): I-variations of the invaginatus process and associated anterior crown forms. Oral Surg Oral Med Oral Pathol. 1957; 10: 1204-1218.
- Cole G, Taintor J, Garth, J. Endodontic therapy of a dilated dens invaginatus. J Endod. 1978;4(3):88-90.
- Rotstein I, Stabholz A, Heling I, Friedman S. Clinical considerations in the treatment of dens invaginatus. Endod Dent Traumatol.1987;3(5):249-254.
- Sousa S, Bramante C. Dens Invaginatus: treatment choices. Endod Dent Traumatol.1998;14(4):152-158.
- Pallavi Reddy Y, Karpagavinayangam K, Subbarao C. Management of dens invaginatus diagnosed by spiral computed tomography: a case report. J Endod. 2008; 34(9):1138-1142.
- Nostrat A, Scheineder C. Endodontic Management of a Maxillary Lateral Incisor with 4 Root Canals and a Dens Invaginatus Tract. J Endod. 2015;41(7):1167-1171.
- Hovland EJ, Block RM. Non-recognition and subsequent endodontic treatment of dens invaginatus. J Endod. 1977;3(9):360-362.
- Ridell K, Mejare I, Matsson L. Dens Invaginatus: a retrospective study of prophylactic invagination treatment. Int J Clin Pediatr Dent. 2001;11(2):92-97.
- Tagger M. Nonsurgical endodontic therapy of tooth invagination. Report of a case. Oral Surg Oral Med Oral Pathol. 1977;43(1):124-129.
- Lindner C, Messer HH, Tyas MJ. A complex treatment of dens invaginatus. Endod Dent Traumatol. 1995;11(3):153-155.
- Hallet GE. The incidence, nature, and clinical significance of palatal invagination in the maxillary incisors teeth. Proc R Soc Med. 1953;46(7):491-499.
- Oehlers FAC. The radicular variety of Dens Invaginatus. Oral Surg Oral Med Oral Pathol. 1958;11(11):1251-1260.
- Agrawal P, Wankhade J, Warhadpande M. A Rare Case of Type III Dens Invaginatus in a Mandibular Second Premolar and Its Nonsurgical Endodontic Management by Using Cone-Beam Computed Tomography: A Case Report. J Endod. 2016;42(4):669-672.
- Patel S. The use of cone beam computed tomography in the conservative management of dens invaginatus: a case report. Int End J. 2010;43:707-713.
- Mishra S, Mishra L, Sahoo SR. A Type III Dens Invaginatus with Unusual Helical CT and Histologic Findings: A Case Report. J Clin Diagn Res. 2012; 9: 1606-1609.
- Kfir A, Telishevsky-Strauss Y, Leitner A, Metzger Z. The diagnosis and conservative treatment of complex Type 3 dens invaginatus using cone-beam computed tomography (CBCT) and 3 plastic models. Int End J. 2013;46(3):275-288.
- Abella F, Teixido LM, Patel S, et al. Cone-bean computed tomography of the root canal morphology of maxillary first and second premolar in the Spanish population. J Endod. 2015;41(8):1241-1247.
- Serota K. Cone-Beam computed tomography: How safe is CBCT for your patients? Dental Economics. January 2011. https://www.dentaleconomics.com/science-tech/article/16394714/cone-beam-computed-tomography-how-safe-is-cbct-for-your-patients. Accessed August 9, 2021.
- Durack C, Patel S. Cone beam computed tomography in endodontics. Braz Dent J. 2012;23(3):179-191.
- Nik-Hussein NN. Dens invaginatus: Complications and treatment of non-vital infected tooth. J Clin Pediatr Dent. 1994;18(4):303-306.
- Chen RJ, Yang JF, Chao TC. Invaginated tooth associated with periodontal abscess. Oral Surg Oral Med Oral Pathol. 1990;69(5):659.
- Ferguson FS, Friedman S, Frazzetto V. Successful apexification technique in an immature tooth with dens in dente. Oral Surg Oral Med Oral Pathol. 1980(4);49:356-359.
- Stamfelj I, Kansky AA, Gaspersic D. Unusual variant of Type 3 dens invaginatus in a maxillary canine: A rare case report. J Endod. 2007;33(1):64-68.
- Pai SF, Yang SF, Lin LM. Nonsurgical endodontic treatment of dens invaginatus with the large periradicular lesion: a case report. J Endod. 2004;30(8):597-600.
- Narayana P, Hartwell G, Wallace R, Nair P. Endodontic clinical management of dens invaginatus case by unique treatment approach. A case report. J Endod. 2012;(38)8:1145-1148.
- Kenee DM, Allemang JD, Johnson JD, Hellstein J, Nichol BK. A quantitative assessment of efficacy of various calcium hydroxide removal techniques. J Endod. 2006;32(6):563-565.
- Lambrianidis T, Kosti E, Boutsioukis C, Mazinis M. Removal efficacy of various calcium hydroxide/chlorhexidine medicaments from the root canal. Int Endod J. 2006;39(1):55-61.
- Pabel AK, Hülsmann M. Comparison of different techniques for removal of calcium hydroxide from straight root canals: an in vitro study. 2017;105:453-459.
- Keshin C, Sariyilmaz E, Sariyilmaz Ö. Efficacy of XP-endo Finisher File in Removing Calcium Hydroxide from Simulated Internal Resorption Cavity. J Endod. 2017;43:(1)126-130.
- Mangani F, Ruddle CJ. Endodontic treatment of a “very particular” maxillary central incisor. J Endod. 1994;20(11):560-561.
Stay Relevant With Endodontic Practice US
Join our email list for CE courses and webinars, articles and more..
