CE Expiration Date:
CEU (Continuing Education Unit): Credit(s)
AGD Code:
Educational aims and objectives
This article aims to show the reader successful management of a case with unusual anatomy of the root canal system of first lower molars.
Expected outcomes
Endodontic Practice US subscribers can answer the CE questions by taking the quiz to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can:
- Recognize the importance of using a cone beam computed tomography to evaluate the
complexity of the morphology of teeth before the endodontic treatment. - Identify the characteristics and types of the middle mesial canal (MMC).
- Recognize that endodontic treatment of mandibular molars requires a high level of knowledge and clinical skills due to their anatomical variations.
- Realize that missed root canals are a possible cause of failure in previous root canal treatment of first lower molars.
- Realize that teeth with atypical canal configuration complicate the process of identifying and accessing root canals in the endodontic treatment.
Drs. Yurii Riznyk and Svitlana Riznyk show how challenges created by atypical anatomy can be overcome with the latest in instrumentation and equipment.
Drs. Yurii Riznyk and Svitlana Riznyk present a challenging case demonstrating the importance of locating all root canals
A 30-year-old female patient presented with symptomatic irreversible pulpitis of both LR6 and LL6 teeth. Cone beam computed tomography (CBCT) of the region revealed a middle mesial canal (MMC) in tooth LR6, and a middle distal canal in tooth LL6. The case was managed with K-Files (Dentsply Maillefer), K-File Nitiflex (Dentsply Maillefer), ProTaper Next® (Dentsply Maillefer), XP-endo® Shaper (FKG), and BT-Race (FKG) under copious irrigation with sodium hypochlorite, ethylenediaminetetraacetic (EDTA) acid, and saline. Premixed bioceramic sealer TotalFill® (FKG) and gutta percha were used for root canal obturation. The access cavities were restored using glass ionomer cement and resin composite. A 12-month review showed that the teeth were functional within normal periodontal parameters. The favorable clinical and radiographic outcome in this case demonstrated that the treatment approach followed is effective in solving complex clinical challenges.
Introduction
The main objective of endodontic therapy is a thorough debridement of the root canal space followed by complete obturation (Vertucci, 2005). The latest advances in the instrumentation techniques and equipment have enabled us to solve difficult clinical cases in endodontics (Berutti, et al., 2009). At the same time, regardless of the continuous improvement in technology, the thorough knowledge of the internal anatomy of the pulp chamber and the root canal system is critical to increasing the rate of clinical success of endodontic treatment (Fava, 2001; Vertucci, 2005). The failure of the treatment could be the result of failure to recognize any unusual canal configuration, as well as prepare and perform the proper obturation of the missed root canals (Leonardo, 1998; Almeida, et al. 2015). This assertion may be confirmed by the research of Song, et al. (2011), who reported that 30% of possible causes of failure in the previous root canal treatment of first lower molars were missed root canals.
In most of the cases, the first mandibular molar has two roots with two root canals in the mesial root and one canal in the distal root (Vertucci, et al., 2006; de Pablo, et al., 2010). In the endodontic treatment of the first mandibular molar, the main difficulty is the mesial root, which may have an additional middle root canal — middle mesial canal (MMC), located in the developmental groove between the mesiolingual (ML) and the mesiobuccal (MB) canals. According to studies, the third canal in the mesial root can be found up to 18% of cases (Pomerantz, et al., 1981; Navarro, et al., 2007; de Pablo, et al., 2010; Versiani, et al., 2016).
The MMC is categorized into three types: Fin, independent, and confluent (Pomerantz, et al., 1981):
- Fin type lacks a separate orifice. It is usually a small linear extension of MB or ML canal.
- A separate orifice and separate apex are specific to this independent type.
- The confluent type is characterized by a separate orifice, but it merges with either the MB or the ML canal.
The research found that confluent configuration is the most prevalent anatomic configuration (Versiani, et al., 2016). Most of the MMC orifices are at the cementoenamel junction (CEJ) level; however, it may also be detected at 1 mm and 2 mm depths from the CEJ and even deeper (Keleş & Keskin, 2017), and may need an additional groove preparation. There are also reports of the presence of three root canals in the distal root, with the incidence of 0.2%-3% (Kottoor, et al., 2010).
Analyzing the morphology of the mesial root, Type IV, according to Vertucci classification, was most often identified — 52.3%, and Type II in 35% of cases (de Pablo, et al., 2010). In the distal root, the most often identified type was Type I — 62.7%, and Type II — 14.5% (de Pablo, et al., 2010).
The usage of the intraoral radiographs, a dental operating microscope, a sharp explorer, and staining with methylene blue dye are commonly accepted principles for primary endodontic treatment (de Carvalho and Zuolo, 2000; Chavda and Garg, 2016). However, radiographs provide a very simple two-dimensional image, hiding the complex structure of root canals, making the evaluation of the morphological structure of the molars complex and challenging. At the same time, the use of 3D analysis has undeniable advantages in the identification of morphological variations of teeth (Durack and Patel, 2012; de Paula, et al., 2013).
Nevertheless, the use of this method is limited for the primary endodontic treatment due to the ALARA principle, which states that every effort should be made by professionals to keep the patient’s exposure to ionizing radiation as low as practically possible (Farman, 2005). In this case report, the preoperative 3D examination and CBCT 1-year after the treatment were not performed for the endodontic treatment of teeth LL6 and LR6, but for the examination, diagnosis, planning, and evaluation of results of surgical treatment on the mandible. The technique enabled to evaluate the complexity of the morphology of lower molars before the endodontic treatment.
Case report
A 30-year-old female patient was referred to the clinic with the chief complaint of spontaneous pain in the lower right region of the jaw for 3 days previous. The patient’s medical and family history was non-contributory. On clinical examination, a deep carious lesion was seen in tooth LR6. Thermal testing of the right mandibular first molar caused intense lingering pain. Percussion and palpation in the region of this tooth were painless, and investigations for sinus tract and periodontal involvement were negative.
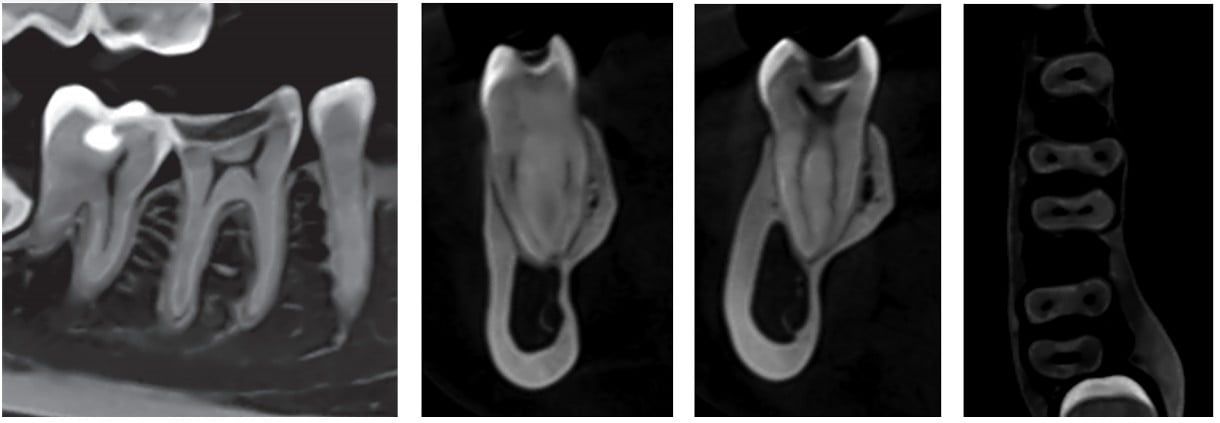
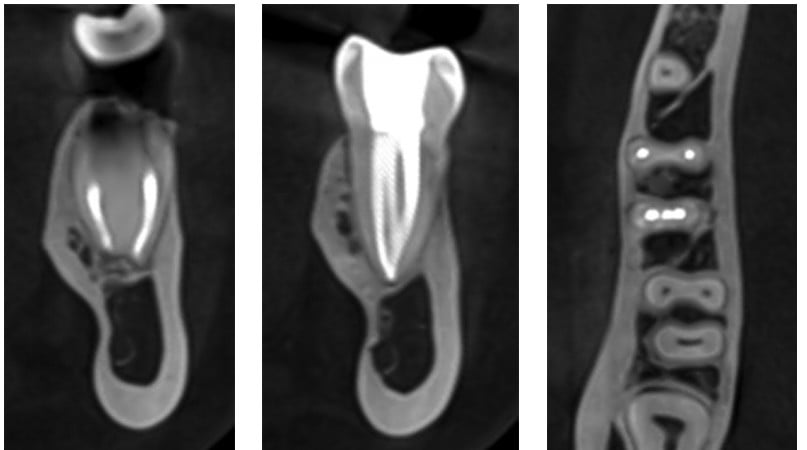
The preoperative sagittal section of CBCT (Figure 1) revealed radiolucency on the occlusal surface of the crown approaching the pulp space in the LR6. The coronal sections of CBCT of the mesial (Figure 2) and distal roots (Figure 3) revealed two root canals in each of them. The axial section (Figure 4) confirmed MMC in the tooth LR6.
A diagnosis of symptomatic irreversible pulpitis was made, based on the clinical and radiographic examination, and we recommended conservative endodontic treatment. The patient declined alternative treatment methods.
After administration of conductive anesthesia (Ubistesin™ 4% 1:100000; 3M Oral Care) and rubber dam isolation of the operative area, we performed access to the pulp chamber using long neck drills and ultrasonic tips. The pulp chamber was rinsed with 6% sodium hypochlorite (NaOCl). We used staining with methylene blue dye and Micro-Opener 15.04 (Dentsply Maillefer) under the optical magnification to examine the pulp chamber floor.
After access preparation and a careful analysis of the floor, we found two root canals in the mesial roots and two root canals in distal ones. The orifice of the MMC was found after the developmental groove preparation by the ultrasonic tip in the mesial root between the previously identified ML and MB canals. It is necessary to remember that diameter of the MMC canal is smaller in comparison with the ML and MB canals, and due to the anatomical danger zones, it requires more careful preparation (De-Deus, et al., 2019; Keles, et al., 2020).
We negotiated canals, and established patency at working length with 10 K-File (Dentsply Maillefer) using an iPex apex locator (NSK, Japan) and confirmed with radiographs. A size 15 K-File Nitiflex (Dentsply Maillefer) was used to perform the glide path. Then we conducted the shaping of the root canals using the ProTaper Next X1 (Dentsply Maillefer) instrument, followed by the XP-endo Shaper (FKG), and 35/.04 BT-Race (FKG). At each change of the endodontic instrument, we irrigated the canals with a 6% NaOCl. For better purification of the isthmus, the Micro-Debriders (Dentsply Maillefer) were used.
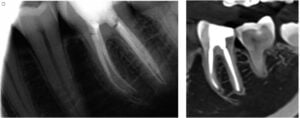
At the end of preparation, we applied 17% ethylenediaminetetraacetic acid (EDTA) for 1 minute to remove the smear layer and performed the irrigation with a copious volume of 6% NaOCl. XP-endo finisher (FKG) was used within 15 seconds to activate all of the solutions, applying slow, gentle longitudinal movements of 7 mm-8 mm to cover the entire length of the canal. Before the obturation, we rinsed all canals with saline. All master cones were processed antiseptically, fitted, and set on a working length. The canals were partially dried with paper points and obturated by cold hydrodynamic obturation technique of gutta percha and premixed bioceramic sealer Totalfill (FKG). We cleaned the pulp chamber in order to remove the excess of gutta percha and bioceramic sealer, temporarily restored the tooth with resin composite, and made the posttreatment radiograph of tooth LR6 (Figure 5). Then we referred the patient for the permanent restoration of tooth LR6.

We were able to evaluate the complexity of the morphology of tooth LR6 and its obturation, with the CBCT (Planmeca ProMax®, Finland) of the mandible 1 year after the treatment (Figures 6-9).
In the medial system, the pulp space separates into three canals, and two of them join into one during its course to exit as two root canals (Figure 7), which are the 3-2 type according to the classification of the root canal morphology (Gulabivala, et al., 2001; Sert and Bayirli, 2004; Bansal, et al., 2018).
In the distal system (Figure 8), two canals run separately from orifice to apex, which corresponds to the Type 2-2 classification of root canals morphology (Vertucci, 1984; Weine, et al., 1988; Bansal, et al., 2018). Axial CBCT slice of tooth LR6 confirmed three root canals in the medial and two root canals in distal roots (Figure 9).
In a short while, the same patient was referred to the clinic with the chief complaint of intermittent moderate pain in the lower-left region of the jaw. On clinical examination, we could see a deep carious lesion in tooth LL6. Pulp thermal testing caused intense, extended pain. The percussion test of the tooth LL6 was negative. The tooth was apically painless to palpation. The periodontal probing near LL6 was within the physiological norm.
A preoperative sagittal section of CBCT (Figure 10) revealed radiolucency on the occlusal surface of the crown, approaching the pulp space in the LL6. The coronal sections of CBCT showed two root canals of the medial root (Figure 11) and two main canals in the distal root (Figure 12). The axial sections (Figure 13) confirmed MDC in the tooth LL6.
All clinical signs indicated the symptomatic irreversible pulpitis, and conservative endodontic treatment was recommended. The patient declined alternative treatment methods, so we carried out the treatment of tooth LL6 according to the same main principle as mentioned above.
After anesthesia (Ubistesin 4% 1:100000; 3M Oral Care) and rubber dam isolation of the operative area, we gained access to the pulp chamber. Then we investigated the bottom of the pulp chamber with Micro-Opener 15.04 (Dentsply Maillefer) under the optical magnification. The pulp chamber was antiseptically processed.
As in the previous case, during the examination of the bottom of the pulp chamber, we found two root canals in the mesial roots and two root canals in distal ones. Based on the CBCT data, we made the preparation of the developmental groove in the distal root between the identified DL and DB canals, and the orifice of the MDC was found approximately 3 mm below the CEJ.
Afterward, we negotiated canals, and established patency at working length with 10 K-File (Dentsply Maillefer) using an iPex apex locator (NSK, Japan) and confirmed with radiographs. A size 15 K-File Nitiflex (Dentsply Maillefer) was used to perform the glide path. The mechanical instrumentation of the root canals was performed using the 10/.06 BT-Race (FKG) instrument followed the XP-endo Shaper (FKG), and 35/.04 BT-Race (FKG) with isthmus cleaning with the Micro-Debriders (Dentsply Maillefer). At each change of instrument, we irrigated the canals with a 6% NaOCl. At the final stage of biomechanical preparation, 17% EDTA was applied for one minute succeeded by the copious amount of 6% NaOCl. To activate the solutions we used the XP-endo Finisher (FKG).
Before the obturation, all canals were rinsed with saline. We processed all master cones antiseptically, then fitted and set them on a working length. The canals were partially dried with paper points, and we carried out the cold hydrodynamic obturation technique of gutta-percha and bioceramic sealer TotalFill (FKG) to obturate them. The cleaning of the pulp chamber was performed, and glass-ionomer cement and resin composite were applied to temporarily restore the tooth. We made the posttreatment radiograph of tooth LL6 (Figure 14). Then the patient was referred for the permanent restoration of tooth LL6.
The patient was recalled at 6 and 12 months postoperatively. At follow-up appointments, the LL6 and LR6 teeth were asymptomatic and functional.
We used the same CBCT (Planmeca ProMax, Finland) of the mandible to evaluate the complexity of the morphology of tooth LL6 and its obturation, 1 year after the treatment (Figures 15-18). In the mesial system, two separate root canals with separate orifices and two separate apexes (Figure 16) correspond to the Type 2-2 morphology of root canals system (Vertucci, 1984; Weine et al., 1988; Bansal et al., 2018).
Distal root canals correspond Type 2-3-1: two canals divide into three and then during its course unite into one (Sert and Bayirli, 2004; Al-Qudah and Awawdeh, 2009; Bansal, et al., 2018). Root canals overlap one another on the postoperative radiograph (Figure 14). Axial slice of CBCT tooth LL6 confirmed two root canals in mesial and three root canals in the distal roots (Figure 18).
Discussion
Endodontic treatment of mandibular molars requires a high level of knowledge and clinical skills due to their anatomical variations. One of the studies claimed that middle mesial canal can be the sequelae of instrumenting the isthmus between the mesiobuccal and mesiolingual canals rather than an extra canal (Mortman and Ahn, 2003). However, according to the more recent studies, the true third canal in the mesial root of the mandibular first molar was found up to 18% (Navarro, et al., 2007; de Pablo, et al., 2010; Versiani, et al., 2016), and 0.2-3% in the distal root (Kottoor, et al., 2010).
Teeth with atypical canal configuration complicate the process of identifying and accessing root canals in the endodontic treatment. CBCT has the ability to overcome the limitations of conventional radiography such as three-dimensional evaluation of the complex canal anatomy during endodontic treatment (Durack and Patel, 2012; de Paula, et al., 2013), but it is necessary to remember that in usual practice, a posttreatment CBCT must be confirmed by appropriate indications and meet with current guidelines regarding ALARA. The dental operating microscope is necessary for the detection of accessory canals in mandibular molars (de Carvalho and Zuolo, 2000; Karapinar-Kazandag, et al., 2010).
At the present stage of the development of endodontics, it is impossible to carry out a complete cleaning of the root canal system. When flat or curved root canals with oval cross sections are considered, the most current rotary nickel-titanium file systems will not adequately clean and shape the canal with favorable results (Metzger, et al., 2010). Therefore, an endodontic file should be used that adapts to the natural morphology of the root canals and efficiently cleans it. Appropriate shaping and cleaning of the root canal system with the XP-endo Shaper and XP-endo Finisher instruments used for this clinical case have the potential to improve root canal system cleaning (Azim, et al., 2016; Azim, et al., 2017).
Conclusion
Professionals should always consider morphological variations of the root canal system before the beginning of treatment. This case report reinforces the importance of using cone beam computed tomography to evaluate the complexity of the morphology of teeth before the endodontic treatment.
The favorable clinical and radiographic outcome in this case demonstrated that the treatment approach followed in the present case is effective in solving complex clinical challenges.
For an interesting article on atypical anatomy on maxillary first premolars, click here: https://endopracticeus.com/ce-articles/treatment-of-maxillary-first-premolars-with-three-root-canals-case-report/
References
- Almeida G, Machado R, Sanches Cunha R, Vansan LP, Neelakantan P. Maxillary first molar with 8 root canals detected by CBCT scanning. Gen Dent. 2015;63(2):68-70.
- Al-Qudah AA, Awawdeh LA. Root and canal morphology of mandibular first and second molar teeth in a Jordanian population. Int Endod J. 2009;42(9):775–784.
- Azim AA, Aksel H, Zhuang T, et al. Efficacy of 4 irrigation protocols in killing bacteria colonized in dentinal tubules examined by novel confocal laser scanning microscope analysis. J Endod. 2016;42(6): 928-934.
- Azim AA, Plasecki L, da Silva Neto UX, Cruz ATG, Azim KA. XP-Shaper, a novel adaptive core rotary instrument: Micro-computed tomographic analysis of its shaping abilities. J Endod. 2017;43(9):1532-1538.
- Bansal R, Hegde S, Astekar MS. Classification of root canal configurations: A review and a new proposal of nomenclature system for root canal configuration. Journal of Clinical and Diagnostic Research. 2018;12(5):1-5.
- Berutti E, Cantatore G, Castellucci A, et al. Use of nickel-titanium rotary PathFile to create the glide path: comparison with manual preflaring in simulated root canals. J Endod. 2009;35(3):408–412.
- Chavda SM, Garg SA. Advanced methods for identification of middle mesial canal in mandibular molars; an in vitro study. 2016;28(2):92-96.
- de Carvalho MC, Zuolo ML. Orifice locating with a microscope. J Endod. 2000;26(9):532-534.
- De-Deus G, Rodrigues EA, Belladonna FG, et al. Anatomical danger zone reconsidered: a micro-CT study on dentine thickness in mandibular molars. Int Endod J. 2019;52(10):1501-1507
- de Pablo OV, Estevez R, Péix Sánchez M, Heilborn C, Cohenca N. Root anatomy and canal configuration of the permanent mandibular first molar: a systematic review. J Endod. 2010;36(12):1919-1931.
- de Paula AF, Brito-Júnior M, Quintino AC, et al. Three independent mesial canals in a mandibular molar: Four-year follow-up of a case using cone beam computed tomography. Case Rep Dent.
- Durack C, Patel S. Cone beam computed tomography in endodontics. Br Dent J. 2012;23(3):179-191.
- Farman AG. ALARA still applies. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005;100(4): 395-397.
- Fava LRG. Root canal treatment in an unusual maxillary first molar: a s case report. Int Endod J. 2001;34(8):649-653.
- Gulabivala K, Aung TH, Alavi A, Ng YL. Root and canal morphology of Burmese mandibular molars. Int Endod J. 2001;34(5):359-370.
- Karapinar-Kazandag M, Basrani BR, Friedman S. The operating microscope enhances detection and negotiation of accessory mesial canals in mandibular molars. J Endod. 2010; 36(8):1289-1294.
- Keleş A, Keskin C. Detectability of middle mesial root canal orifices by troughing technique in mandibular molars: a micro–computed tomographic study. J Endod. 2017;43(8):1329-1331.
- Keleş A, Keskin C, Alqawasmi R, Versiani M. Evaluation of dentine thickness of middle mesial canals of mandibular molars prepared with rotary instruments: a micro-CT study. Int Endod J. 2020;53(4):519-528.
- Kottoor J, Sudha R, Velmurugan N. Middle distal canal of the mandibular first molar: a case report and literature review. Int Endod J. 2010;43(8):714-722.
- Leonardo MR. Aspectos anatomicos da cavidade pulpar: relacoes com o tratamento de canais radiculares. In: Leonardo MR, Leal JM eds. Endodontia: tratamento de canais radiculares. 3rd ed. São Paulo: Panamericana; 1998.
- Metzger Z, Zary R, Cohen R, Teperovich E, Paque F. The quality of root canal preparation and root canal obturation in canals treated with rotary versus self-adjusting files: a three-dimensional micro-computed tomographic study. J Endod. 2010;36(9):1569-1573.
- Mortman RE, Ahn S. Mandibular first molars with three mesial canals. Gen Dent. 2003;51(6):549-551.
- Navarro LF, Luzi A, Garcia AA, Garcia AH. Third canal in the mesial root of permanent mandibular first molars: review of the literature and presentation of three clinical reports and two in vitro studies. Med Oral Patol Oral Cir Bucal. 2007;12(8):605-609.
- Pomerantz HH, Eidelman DL, Goldberg MG. Treatment considerations of the middle mesial canal of mandibular first and second molar. J Endod. 1981;7(12):565-568.
- Sert S, Bayirli GS. Evaluation of the root canal configurations of the mandibular and maxillary permanent teeth by gender in the Turkish population. J Endod. 2004;30(6):391-398.
- Song M, Kim HC, Lee W, Kim E. Analysis of the cause of failure in nonsurgical endodontic treatment by microscopic inspection during endodontic microsurgery. J Endod. 2011;37(11):1516-1519.
- Versiani MA, Ordinola-Zapata R, Keleş A, et al. Middle mesial canals in mandibular first molars: a micro-CT study in different populations. Arch Oral Biol. 2016;61:130-137.
- Vertucci F. Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol. 1984; 58(5):589-599.
- Vertucci FJ. Root canal morphology and its relationship to endodontic procedures. Endod Topics. 2005;10:3-29.
- Vertucci FJ, Haddix JE, Britto LR. Tooth morphology and access cavity preparation. In: Cohen S, Hargreaves KM, eds. Pathways of the pulp. 9th ed. St. Louis MO: Mosby; 2006.
- Weine FS, Pasiewicz RA, Rice RT. Canal configuration of the mandibular second molar using a clinically oriented in vitro method. J Endod. 1988;14(5):207-213.
Stay Relevant With Endodontic Practice US
Join our email list for CE courses and webinars, articles and more..
