CE Expiration Date: October 5, 2028
CEU (Continuing Education Unit):2 Credit(s)
AGD Code: 070
Educational aims and objectives
This self-instructional course for dentists aims to examine the significant role of the lateral canal’s various morphological, topographical, and clinical aspects that contribute to effective endodontic therapy.
Expected outcomes
Endodontic Practice US subscribers can answer the CE questions by taking the quiz online at endopracticeus.com to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can:
- Identify the physical characteristics of the lateral canal.
- Recognize the difficulty of instrumenting and irrigating lateral canals efficiently.
- Realize some efficient ways to improve obturation of lateral canals.
- Realize some reasons for encountering complications during treatment of the lateral canal.
Drs. Juan Pablo Miraglia Cantarini, Denise Alfie, Gonzalo García, Carlos Cantarini, and Fernando Goldberg discuss a study on the complexities and complications of the lateral canal and its importance in the root canal system.
Drs. Juan Pablo Miraglia Cantarini, Denise Alfie, Gonzalo García, Carlos Cantarini, and Fernando Goldberg study a condition that poses complex challenges
Abstract
Introduction: The lateral canal (LC) is a crucial communication pathway between the root canal system and the periodontal tissues. LC cleaning poses challenges during endodontic treatment due to its complexity, which can lead to complications such as lateral lesions even without apical pathology.
Materials and methods
This study analyzed radiographs of 272 teeth undergoing endodontic treatment or retreatment to detect obturated LCs. The teeth were categorized by root third location, presence of lateral pathology, and specific root involvement in multi-rooted teeth. A subset of 136 teeth was evaluated clinically and radiographically over intervals up to 10 years. Various obturation techniques and sealers were also evaluated.
Results
Of the 272 cases, 237 had a single LC, primarily in the apical third. In 35 cases, two LCs were detected. Long-term follow-ups revealed higher repair rates with extended observation, with an 83% success rate after 2 years. Retreatment was not a statistically significant factor for incomplete repair. This means that there was no clear evidence showing that retreatment influenced the chance of the problem being fixed.
Conclusion
LCs play a significant role in endodontic prognosis due to their potential to harbor necrotic tissue. Thermoplasticized gutta-
percha techniques showed the highest success rate in obturating LCs, especially in primary treatments. Long-term follow-ups are crucial for confirming successful repair.
Introduction
The lateral canal (LC) represents a crucial pathway of communication between the root canal system and the surrounding periodontal tissue. In endodontic treatments, the LC contains vital tissue, and under certain circumstances, the cleaning and shaping process itself may lead to intraoperative bleeding, which can complicate and occasionally alter the subsequent obturation. LCs can vary in caliber and, in some cases, extend beyond the apical foramen.
It is evident that bacterial progression from the coronal area due to carious tissue affects the LC first before reaching the apical foramen. Thus, radiographically, a lateral lesion without an apical lesion can be observed. Furthermore, a lateral lesion may originate from an LC where the vital tissue has been destroyed by septic pulp necrosis, yet vital pulp can still be found. According to Ricucci and Siqueira Jr.,1 when the caliber of the LC is wide, it can contain a significant amount of necrotic tissue and bacteria. Radiographically, obturated LCs are only perceptible when located along the proximal walls; if they are vestibular, palatal, or lingual, they overlap with the radiopacity of the endodontic obturation and are not visible on the radiograph. Galvão Barbosa, et al.,2 observed in an ex vivo study on mandibular molars that most LCs were detected on the lingual, vestibular, distolingual, and distobuccal surfaces.
Cleaning of LCs cannot be achieved with endodontic instruments; only irrigation solutions can fulfill this function. Wang, et al.,3 highlight the difficulty in ensuring irrigation solution reaches the entirety of the LC, regardless of the type of irrigation needle used.1 Additionally, LCs are unlikely to be completely clean after instrumentation and irrigation, irrespective of the technique or solution used. Several authors suggest that removing the smear layer from the dentinal walls post-instrumentation increases the likelihood of obturating LCs.4-7 Likewise, the use of agitation of irrigating solutions at the end of the endodontic procedure could lead to a higher frequency of obturated LCs.8-10
On the other hand, the use of calcium hydroxide medication between treatment sessions impedes LC obturation, as remnants can obstruct their pulp entrance.11 The obturation of an LC allows us to confirm the presumed diagnosis of lateral radiolucency and acts as a patency file, expelling septic content from the LC towards the periodontal area, where defenses can minimize its effects. Motamedi and Gilbert10 emphasize that LC obturation can confirm the endodontic origin of the lesion and validate sufficient LC cleaning to allow passage of obturation material through it.
Considering their location, LCs can be found in any of the root thirds, can be singular or multiple, and in their various courses, they cross dentin and dental cementum before reaching the periodontium.
Purpose
The purpose of this article is to analyze various morphological, topographical, and clinical aspects that contribute to the importance of LCs in endodontic therapy.
in the same tooth
Materials and methods
Radiographs of 272 different dental pieces with endodontic treatment or retreatment were observed to identify obturated LCs. The following aspects were individually identified: number, root third location, presence or absence of lateral pathology, and for multi-rooted teeth, the specific root affected. Of these 272 dental pieces, 136 were clinically and radiographically evaluated at different intervals: 49 within 2 years, 43 from 2 to 5 years, 32 from 5 to 10 years, and 12 over 10 years. Clinical and radiographic evaluations at various intervals were conducted based on parameters suggested by Friedman and Mor.
The analyzed dental pieces were represented as follows: Upper Maxilla: Central incisors 45, Lateral incisors 14, Canines 12, Premolars 62, and Molars 18. Lower Maxilla: Central incisors 0, Lateral incisors 3, Canines 7, Premolars 52, and Molars 59. Of all cases, 213 obturated LCs corresponded to endodontic treatments and 59 to non-surgical retreatments.
Seventy-five did not show periradicular radiolucency, while 197 did.
The obturation technique and sealer used were determined for all endodontic treatments. System B™ (n = 113), Hybrid Technique (n = 53), GuttaCore® (n = 35), Lateral Compaction (n = 30), Injectable Gutta-Percha Systems (n = 26), Thermafil® (n = 15). Sealers with resin bases were used in 203 cases, zinc oxide-eugenol-based sealers in 46, bioceramic in 20, and calcium hydroxide-based sealers in 3.
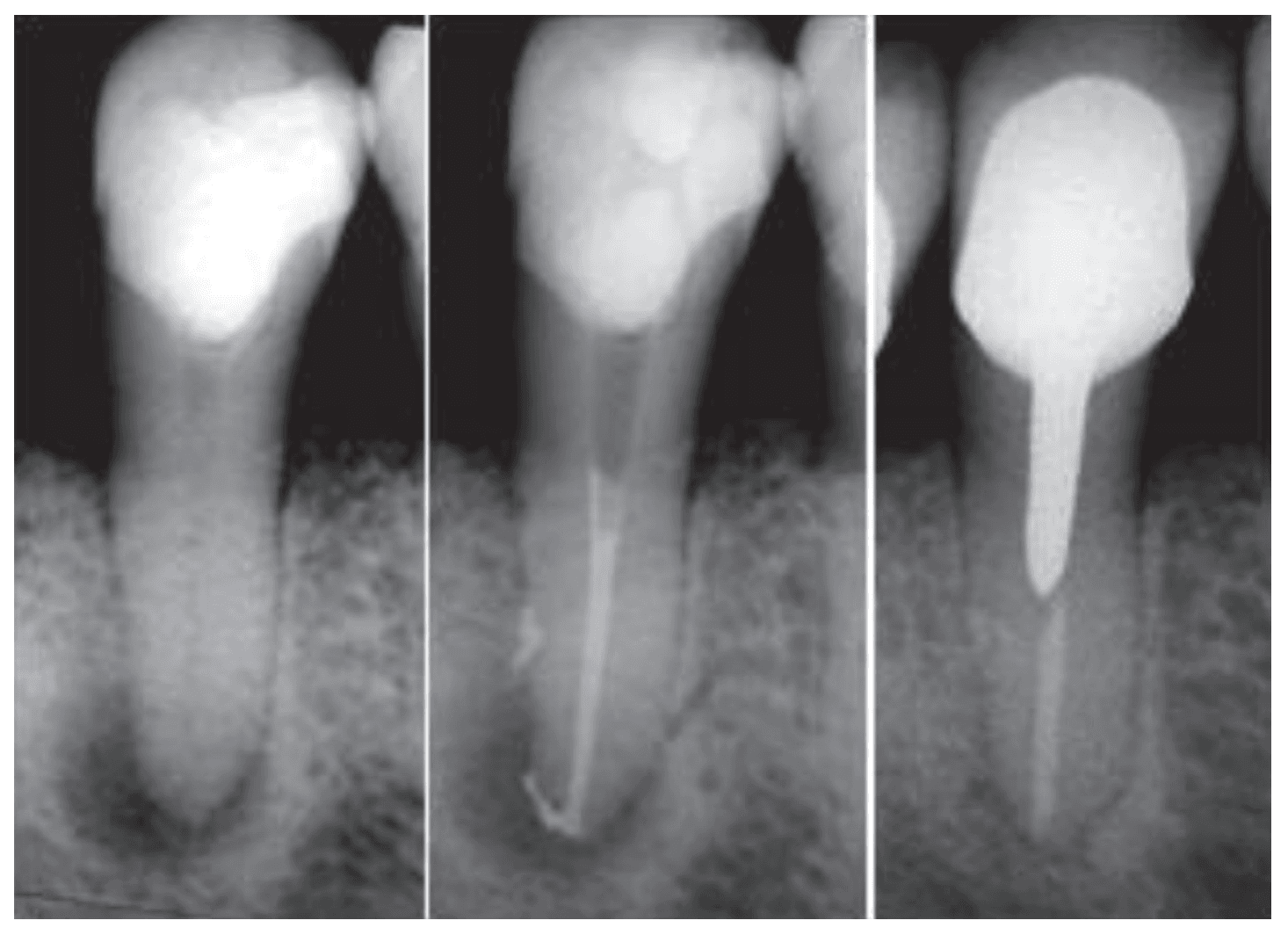
third: a significant periapical radiolucent area is observed. Long-term postoperative image (4 years and 1 month) showing lesion repair with new bone formation
Results
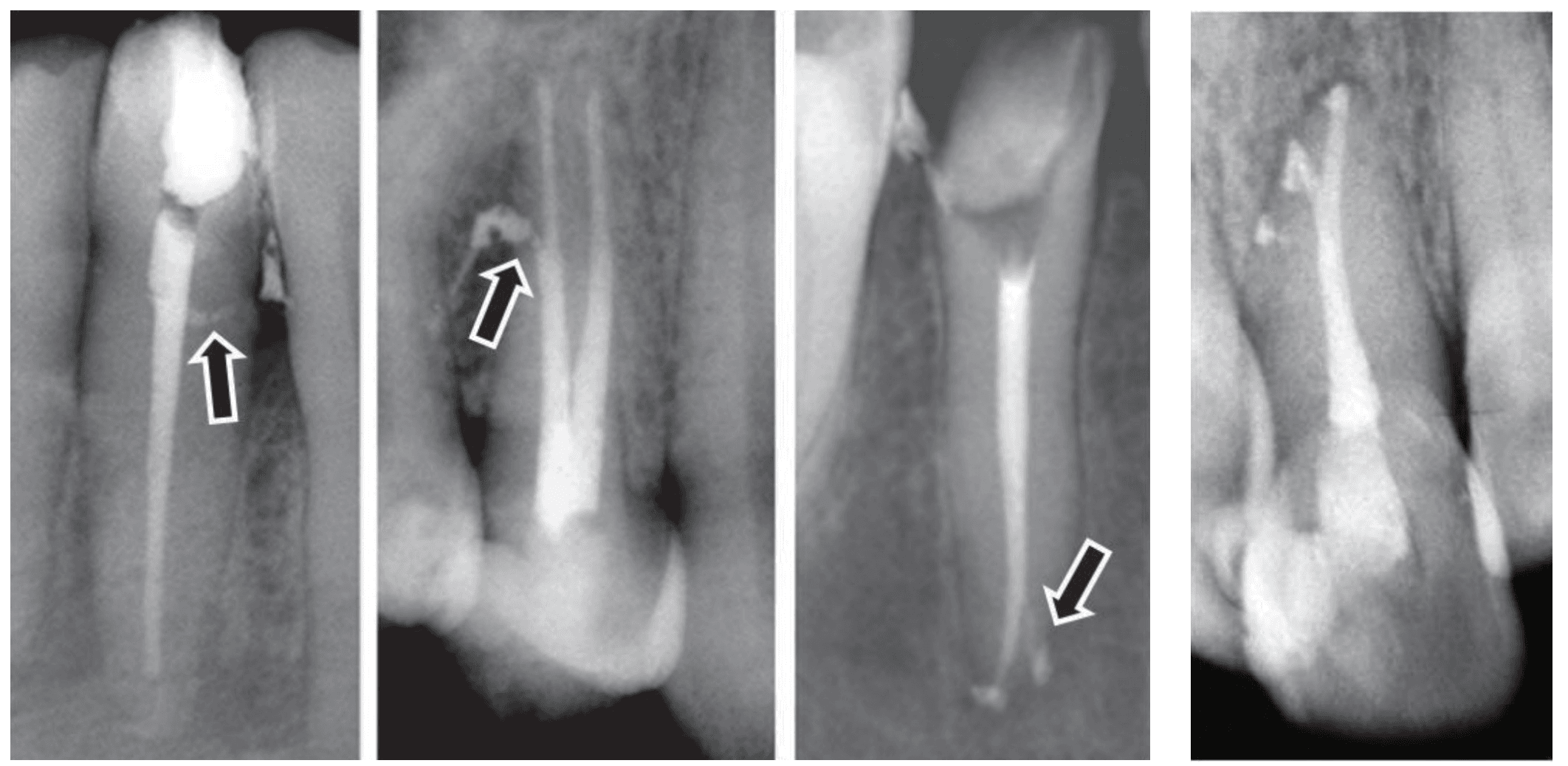
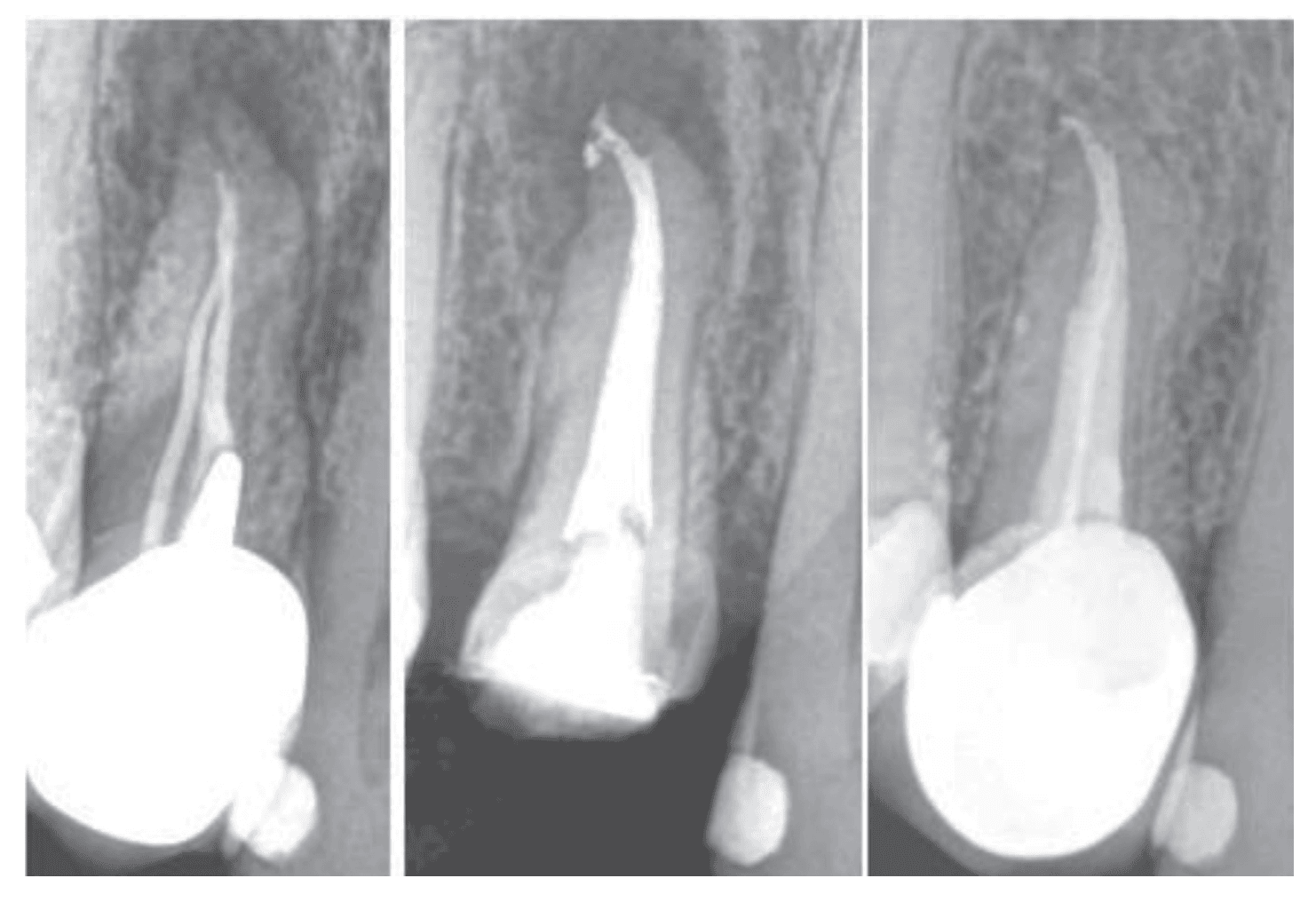
In 237 out of 272 cases, a single LC was present, with 23 located in the coronal third, 83 in the middle third, and 131 in the apical third (Figure 1). In 35 dental pieces, two obturated LCs were detected, with 16 located in the middle and apical thirds, 4 in both middle thirds, and 15 in both apical thirds (Figure 2).
Among the 136 dental pieces with distance evaluations, 92 showed persistent sealer in the LC, while 44 did not.
Of the 59 lower molars, 40 had LCs in the mesial root and 18 in the distal root, with 1 case showing double obturated LCs: one in the mesial and one in the distal root. Among the 18 upper molars, 6 had LCs in the mesio-vestibular root, 9 in the palatal root, 2 in the distobuccal root, and 1 double LC located in the palatal and distobuccal roots.
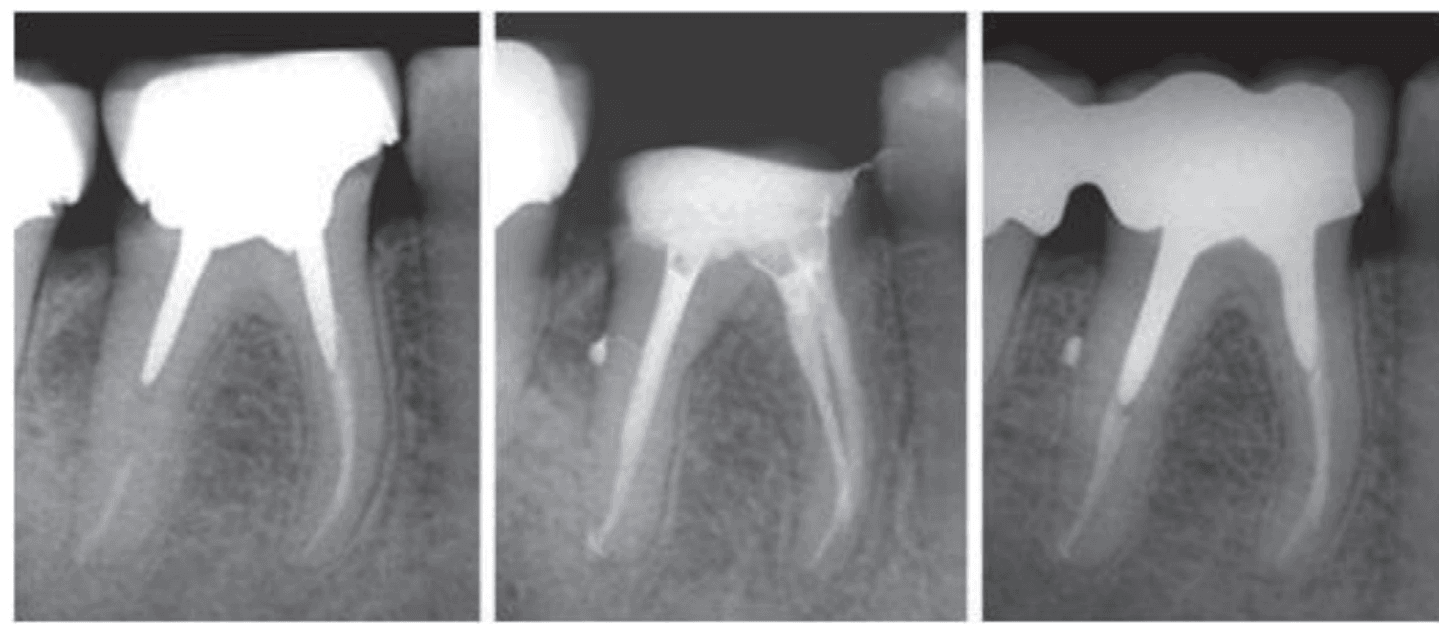
Of the 136 dental pieces with distance evaluations, 49 evaluated within 2 years showed 27 with total repair, 21 in repair, and 1 case with no repair radiographically. Of the 43 evaluated from 2 to 5 years, 36 showed total repair (Figure 3), 6 in repair, and 1 case with no repair. Of the 32 evaluated from 5 to 10 years, 27 showed total repair (Figure 4) and 5 in repair. Of the 12 evaluated over 10 years, 10 showed total repair (Figure 5) and 2 a partial repair.
showing obturation of a lateral canal in the middle third. Long-term postoperative
image (13 years and 8 months) with lesion repair
The chi-squared value (with continuity correction) is 1.02, with a corresponding p-value of 0.31. Therefore, the association between the defined variables cannot be considered statistically significant.
The odds ratio is 2.35, with a corresponding confidence interval of 0.17–8.34. Since this interval includes one, it cannot be considered that retreatment represents a statistically significant risk factor for the absence of complete repair. This means that the confidence interval shows no significant link between retreatment and the problem being fixed, as it includes the value one, which implies no effect.
“When dental pulp undergoes pathology involving microorganisms, lateral canals provide a direct pathway for these microorganisms to affect the periodontal tissue, inevitably leading to periapical pathologies.”
Discussion
When dental pulp undergoes pathology involving microorganisms, LCs provide a direct pathway for these microorganisms to affect the periodontal tissue, inevitably leading to periapical pathologies. Given that LCs can be found in any of the three root thirds, periodontal damage can occur in different areas of the surrounding periodontium. De Deus13 noted in an ex vivo study of 1,140 dental pieces that 27.4% had LCs, with 17.0% located in the apical third, 8.8% in the middle third, and 1.6% in the cervical or coronal third. Similarly, in this study of 272 dental pieces with LCs, 237 were singular, with 9.7% located in the cervical or coronal third, 35% in the middle third, and 55.3% in the apical third. This is in accordance with De Deus’ findings, where the majority of LCs were located apically, followed by the middle and cervical or coronal thirds. Kasahara et al.,14 evaluated 503 maxillary central incisors ex vivo, with over 60% showing LCs, 80% with a caliber close to #10, and 3% with a caliber greater than #40. Among all incisors evaluated, 47.3% had one LC, 25.1% had two, and 13.1% had three. Venturi, et al.,15 observed in an ex vivo study on different dental pieces that most LCs were smaller than 50 um, with some ranging from 50 to 100 um.
According to these authors, vertical gutta-percha compaction resulted in excellent obturation, particularly in LCs located more than 3 mm from the apex. Ricucci and Siqueira1 noted that wide LCs can contain significant amounts of necrotic tissue and bacteria, leading to lateral lesions. Rotstein and Simon16 observed the presence of a lateral cyst originating from an LC emerging from the main canal with infected pulp.
Furthermore, proper endodontic treatment aims to restore periodontal health and thereby replenish lateral bone lost due to pathology. For instance, of the 136 repaired cases presented, various obturation techniques and sealers were employed. Within 2 years of postoperative clinical and radiographic control, they showed a success rate of 55%; however, this exceeded 83% in controls lasting longer than 2 years. Consequently, shorter-term controls exhibited lower success rates compared to longer-term controls, consistent with other authors’ findings.17,18
Regarding the obtained chi-squared statistic, it can be considered that retreatment does not represent a statistically significant risk factor for the absence of complete repair. This means that the chi-squared test results suggest that retreatment is not likely to impact whether repairs are fixed in a statistically significant way.
Regarding the persistence of sealer in the periradicular area adjacent to the obturated lateral canal, it is important to highlight that overfilling may be one of the causes of delayed repair but does not prevent it.18
Several publications indicate that thermoplasticized gutta-percha techniques achieve LC obturation more frequently than lateral compaction techniques, owing to softened gutta-percha exerting more intense pressure against the dentinal walls and root canal intricacies.19,20 Similarly, LC obturation was more frequent in initial treatments compared to retreatments, likely due to persistent remnants from the primary obturation obstructing LC entry.21 Removing primary obturation material completely during retreatment is often challenging.22,23
It is crucial to note that when intraradicular posts are used, preventing an interface between endodontic obturation and the post is essential. Improper post space utilization, as noted by Weine,24 can lead to lateral lesions through an LC with tissue degradation. This remarks the importance of careful post cementation, as they are not sterile and likely contains signs of bacterial contamination that can diffuse through an LC.
Conclusions
Lateral canals (LCs) are anatomical variations of the root canal system that can be found in different root thirds, with varying calibers and courses. Clinically, they become critically important in septic pulp mortifications as they serve as significant bacterial pathways that can damage the surrounding periodontal tissue. Regarding prognosis, there is a clear emphasis on the necessity for extended follow-up periods in many cases until radiographically repair is detected.
Acknowledgments: The authors express their sincere appreciation to Professor Ricardo L. Macchi for his help with the statistical analysis.
Editor’s note: We are sorry to report that Dr. Fernando Goldberg died on April 18, 2025 after an illness. We extend our sincere condolences to his family and colleagues.
Dr. John West also explored the significance of the lateral canal in his article: “Do lateral canals really matter?” Read part 6 of his series here: https://endopracticeus.com/5181/.
References
- Ricucci D, Siqueira JF Jr. Fate of the tissue in lateral canals and apical ramifications in response to pathologic conditions and treatment procedures. J Endod. 2010 Jan;36(1):1-15.
- Barbosa FO, Gusman H, Pimenta de Araújo MC. A comparative study on the frequency, location, and direction of accessory canals filled with the hydraulic vertical condensation and continuous wave of condensation techniques. J Endod. 2009 Mar;35(3):397-400.
- Wang R, Shen Y, Ma J, Huang D, Zhou X, Gao Y, Haapasalo M. Evaluation of the Effect of Needle Position on Irrigant Flow in the C-shaped Root Canal Using a Computational Fluid Dynamics Model. J Endod. 2015 Jun;41(6):931-936.
- Goldberg F, Massone JE, Spielberg C. Effect of irrigation solutions on the filling of lateral root canals. Endod Dent Traumatol. 1986 Apr;2(2):65-66.
- Villegas JC, Yoshioka T, Kobayashi C, Suda H. Obturation of accessory canals after four different final irrigation regimes. J Endod. 2002 Jul;28(7):534-536.
- Shahravan A, Haghdoost AA, Adl A, Rahimi H, Shadifar F. Effect of smear layer on sealing ability of canal obturation: a systematic review and meta-analysis. J Endod. 2007 Feb;33(2):96-105.
- Goldberg F, Artaza LP, Alfie D. Capacity of different irrigation procedures to remove smear layer from the pulpal orifice of simulated lateral canals. Rev Asoc Odontol Argent. 2010;98(2):113-118.
- de Gregorio C, Estevez R, Cisneros R, Paranjpe A, Cohenca N. Efficacy of different irrigation and activation systems on the penetration of sodium hypochlorite into simulated lateral canals and up to working length: an in vitro study. J Endod. 2010 Jul;36(7):1216-1221.
- Kanter V, Weldon E, Nair U, Varella C, Kanter K, Anusavice K, Pileggi R. A quantitative and qualitative analysis of ultrasonic versus sonic endodontic systems on canal cleanliness and obturation. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011 Dec;112(6):809-813.
- Motamedi MRK, Gilbert BE. The lateral puff in endodontics: clinically significant or a storyteller of anatomy and etiology?- A case report series. Endod Pract US. 2023;16(4):22-25.
- Goldberg F, Artaza LP, De S. Influence of calcium hydroxide dressing on the obturation of simulated lateral canals. J Endod. 2002 Feb;28(2):99-101.
- Friedman S, Mor C. The success of endodontic therapy–healing and functionality. J Calif Dent Assoc. 2004 Jun;32(6):493-503.
- De Deus QD. Frequency, location, and direction of the lateral, secondary, and accessory canals. J Endod. 1975 Nov;1(11):361-366.
- Kasahara E, Yasuda E, Yamamoto A, Anzai M. Root canal system of the maxillary central incisor. J Endod. 1990 Apr;16(4):158-161.
- Venturi M, Di Lenarda R, Prati C, Breschi L. An in vitro model to investigate filling of lateral canals. J Endod. 2005 Dec;31(12):877-881.
- Rotstein I, Simon JH. Diagnosis, prognosis and decision-making in the treatment of combined periodontal-endodontic lesions. Periodontol 2000. 2004;34:165-203.
- Molven O, Halse A, Fristad I, MacDonald-Jankowski D. Periapical changes following root-canal treatment observed 20-27 years postoperatively. Int Endod J. 2002 Sep;35(9):784-790.
- Fristad I, Molven O, Halse A. Nonsurgically retreated root filled teeth–radiographic findings after 20-27 years. Int Endod J. 2004 Jan;37(1):12-18.
- DuLac KA, Nielsen CJ, Tomazic TJ, Ferrillo PJ Jr, Hatton JF. Comparison of the obturation of lateral canals by six techniques. J Endod. 1999 May;25(5):376-380.
- Goldberg F, Artaza LP, De Silvio A. Effectiveness of different obturation techniques in the filling of simulated lateral canals. J Endod. 2001 May;27(5):362-364.
- Goldberg F, Artaza LP, García C, Briseño-Marroquín B. Obturation frequency of simulated lateral canals during primary treatment and following re-treatment. Endod Pract Today. 2011;5(2):139-144.
- Rossi-Fedele G, Ahmed HM. Assessment of Root Canal Filling Removal Effectiveness Using Micro-computed Tomography: A Systematic Review. J Endod. 2017 Apr;43(4):520-526.
- De-Deus G, Belladonna FG, Zuolo AS, Cavalcante DM, Simões Carvalho M, Marinho A, Souza EM, Lopes RT, Silva EJNL. 3-dimensional Ability Assessment in Removing Root Filling Material from Pair-matched Oval-shaped Canals Using Thermal-treated Instruments. J Endod. 2019 Sep;45(9):1135-1141.
- Weine FS. The enigma of the lateral canal. Dent Clin North Am. 1984 Oct;28(4):833-852.
Stay Relevant With Endodontic Practice US
Join our email list for CE courses and webinars, articles and more..
