Dr. Antonis Chaniotis discusses the tactile-controlled activation technique using controlled-memory files for severely curved and challenging canals
The ultimate biologic objective of endodontic therapy is the prevention of periradicular disease and the promotion of healing when disease is already established. Arguably, mechanical instrumentation and chemical disinfection of the root canal system are considered the foundational principles for the successful accomplishment of these objectives (Schilder, 1974). Although these principles cannot be considered separately, canal preparation is the essential phase that will determine the efficacy of all subsequent procedures (Peters, 2004).
Traditionally, for gutta-percha fillings, root canal shaping should satisfy specific design objectives:
- The shape of the main root canal should resemble a continuously tapering funnel from the orifice to the apex.
- The cross-sectional diameter of the main canals should be narrower at every point apically.
- Canal preparation should follow the shape of the original root canal.
- The original position of the apical foramen should be preserved.
- The apical opening should retain its original dimensions as much as possible (Schilder, 1974; Hulsmann, Peters, Dummer, 2005).
The biological objectives of root canal instrumentation consist of:
- the confinement of instrumentation to the limits of the roots themselves
- the avoidance of extruding necrotic debris into the periradicular tissues
- the removal of all organic tissue from the main canals as well as from the lateral extent of the root canal system
- the creation of sufficient space to allow irrigation and medication by simultaneously preserving enough circumferential dentin for the tooth to function (Hulsmann, Peters, Dummer, 2005)
Achieving these objectives in straight canals is considered a simple and straightforward procedure with all instrumentation systems available today. The problems of biomechanical instrumentation arise when the internal anatomy of human teeth is severely curved or even bifurcated and anastomotic (Figure 1). In such teeth, the accepted basic endodontic techniques and instrumentation protocols might be challenging to follow.
The aim of this article is to describe the application of tactile-controlled activation (TCA) technique with controlled-memory files for the safer and more predictable instrumentation of severely curved and challenging canals.

The challenge of curved canal management
The internal anatomy of human teeth can be extremely complicated. Based on canal curvature, Nagy, et al., 1995, classified root canals into four categories: straight or I-form (28% of the root canals), apically curved or J-form (23% of the root canals), entirely curved or C-form (33% of the root canals), and multicurved or S-form canals (16% of the root canals). Schäfer, et al., 2002, found that 84% of the human root canals studied were curved and 17.5% of them presented a second curvature and were classified as S-shaped root canals. From all curved canals studied, 75% had a curvature of less than 27º, 10% had a curvature with an angle between 27º and 35º, and 15% had severe curvature of more than 35º.
Traditionally, root canal curvatures were assessed by using the Schneider angle of curvature concept (Schneider, 1971). According to Schneider (1971), root canals presenting an angle of 5º or less could be classified as straight canals, root canals presenting an angle between 10º and 20º as moderate curved canals, and root canals presenting a curve greater than 25º as severely curved canals.
Many decades later, Pruett, et al., 1997, reported that two curved root canals might have the same Weine angle of curvature but totally different abruptness of curvature. In order to define the abruptness of curvature, they introduced the concept of the radius of curvature. The radius of curvature is the radius of a circle passing through the curved part of the canal. The number of cycles before failure for rotary endodontic instruments significantly decreased as the radius of curvature decreased and the angle of curvature increased.
Further attempts to describe mathematically and unambiguously root canal curvatures in two-dimensional radiographs introduced parameters such as the length of the curved part of the canal (Schäfer, et al., 2002) and the location of the curve as defined by curvature height and distance (Günday, Sazak, Garip, 2005).
Estrela, et al., 2008, described a method to determine the radius of root canal curvatures using CBCT images analyzed by specific software. Radius of canal curvatures was classified into three categories: small radius (r≤4mm), intermediate radius (r>4 and r≤8mm) and large radius (r>8mm). The smaller the radius of a curvature, the more abrupt it becomes.
All these attempts to describe the parameters of root canal curvature had one common denominator, the preoperative risk assessment for transportation and unexpected instrument separation.
The risks of canal transportation and instrument separation
According to the AAE Glossary of Endodontic Terms (2012), transportation is defined as the “removal of the canal wall structure on the outside curve in the apical half of the canal due to the tendency of the files to restore themselves to their original linear shape.” For stainless steel hand files and conventional nickel-titanium hand or engine-driven files, the restoring force of a given instrument is directly related to its size and taper. The bigger the size or taper of a given file, the bigger the restoring force becomes due to the increase of the metal mass of the instrument.
If root canals were constructed precisely on the dimensions of our instruments, then transportation wouldn’t be a problem, and our instruments would be well constrained inside the root canal trajectories. Unfortunately, instruments are not well constrained by the canal in a precise trajectory because instruments are not precisely shaped to fit the canal dimensions. As a result, each instrument may follow its own trajectory inside a curved canal guided by its restoring force and transporting the canal (Plotino, et al, 2010). Usually, the greater increase in apical enlargement is targeted in curved canals, the more excessive the dentin removal toward the outer apical curve becomes (Elayouti, et al., 2011) and the more excessive the inner curvature (danger zone) widening can get.
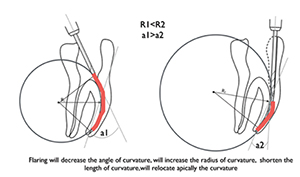
In order to avoid these complications, the more severe the canal curvature, the more we tend to increase flaring and reduce the apical instrumentation size (Roane, Clement, Carnes, 1985). Increasing flaring under such circumstances would result in the reduction of the angle of curvature, in shortening the length of curvature, in increasing the radius of curvature, and in relocating the curvature apically (Figure 2). Smaller apical preparations in highly curved canals would be preferable for two reasons:
- Smaller diameter preparations are related to less cutting of the canal walls, less file engagement, and, consequently, a lesser likelihood for the expression of undesirable cutting effects.
- Small diameter files are more flexible and fatigue resistant, and, therefore, less likely to cause transportation during enlargement (Roane, Clement, Carnes, 1985).
The aforementioned instrumentation approaches, although safer, have inherent disadvantages. Unfortunately, flaring the canal entrance in order to achieve easier negotiation to the apical third of curved canals will result in unnecessary removal of dentin from a level that is considered irreplaceable. Moreover, smaller apical preparations may result in increased difficulties for the irrigation solutions to be delivered to an appropriate canal depth. In highly curved canals, the ability of irrigation solutions to be delivered to the critical apical third depends directly on the ability of our instruments to create adequate apical preparations and on the selection of the appropriate delivery techniques
(Boutsioukis, et al., 2010).
Achieving adequate apical preparations for disinfection without over-flaring the coronal part of highly curved canals is one of the greatest challenges in endodontic instrumentation. This is very true especially under the current concepts of dentin preservation in endodontics.
Achieving adequate apical preparations
for disinfection without over-flaring the coronal part
of highly curved canals is one of the greatest challenges
in endodontic instrumentation
Moreover, the risk of unexpected instrument separation of engine-driven nickel-titanium files poses significant problems during curved canal management. There are two mechanisms that have been implicated with engine-driven instrument fracture — cyclic fatigue and torsional failure. As an engine-driven instrument is activated inside a curved canal, continuous tensile and compressive stresses at the fulcrum of the curvature may lead to instrument separation because of cyclic fatigue. If the tip of an engine-driven instrument is locked inside a canal, and the shaft of the instrument keeps on moving, it may exceed an applied shear moment, resulting in torsional failure. Usually during curved canal management, both mechanisms can co-exist. As the complexity of the curvature increases, the number of cycles before failure decreases for a given instrument, making complicated canal management a real clinical challenge.
Controlled-memory files to minimize instrumentation risks
Nickel-titanium alloys are softer overall than stainless steel, have a low modulus of elasticity (about one-fourth to one-fifth that of stainless steel), greater strength, are tougher and more resilient, and show shape memory and superelasticity (Baumann, 2004). The nickel-titanium alloys used in root canal treatment contain approximately 56% (wt) nickel and 44% (wt) titanium (Walia, Brantley,
Gernstein, 1988). They can exist in two different temperature-dependent crystal structures (phases) called martensite (low-temperature phase, with a monoclinic B19’ structure) and austenite (high temperature or parent phase, with the B2 cubic crystal structure). The lattice organization can be transformed from austenitic to martensitic and return again to austenitic phase by adjusting temperature and stress. During this reverse transformation, the alloy goes through an unstable intermediate crystallographic phase called R-phase.
Preparation of the root canal causes stress to nickel-titanium files, and a stress-induced martensitic transformation takes place from the austenitic phase of conventional nickel-titanium files to the martensitic phase within the speed of sound. A change in shape occurs, together with volume and density changes.
This ability of resisting stress without permanent deformation — going back to the initial lattice form — is called superelasticity. Superelasticity is most pronounced at the beginning of the applied stress when a first deformation of as much as an 8% strain can be totally overcome. After 100 deformations, the tolerance is about 6%, and after 100,000 deformations, it is about 4%. Within this range, the so-called “memory effect” can be observed (Baumann, 2004).
Besides the stress-induced martensitic transformation, the lattice organization of nickel-titanium alloys can be altered also with temperature change. When a conventional nickel-titanium austenitic microstructure is cooled, it begins to change into martensite. The temperature at which this phenomenon begins is called the martensite start temperature (Ms). The temperature at which martensite is again completely reverted is called the martensite transformation finish temperature (Mf). When martensite is heated, it begins to change into austenite. The temperature at which this phenomenon begins is called the austenite transformation start temperature (As). The temperature at which this phenomenon is complete is called the austenite finish temperature (Af), which means that at and above this temperature, the material will have completed its shape memory transformation and will display its superelastic characteristics (Shen, et al., 2011).
Before 2011, the Af temperature for the majority of the available nickel-titanium endodontic instruments was at or below room temperature. As a result, conventional nickel-titanium endodontic instruments were in the austenitic phase during clinical use (body temperature), showing shape memory and superelasticity. In 2011, so-called controlled-memory files were introduced in endodontics. These files had been manufactured utilizing a thermomechanical processing that controls the material’s memory, making the files extremely flexible and fatigue resistant but without the shape memory and restoring force of other nickel-titanium files (Coltene/Whaledent, 2012).
The Af transformation temperature of controlled-memory files is found to be clearly above body temperature. As a result, these files are mainly in the martensite phase in body temperature (Shen, et al., 2011). When the material is in its martensite form, it is soft, ductile, without shape memory, can easily be deformed, yet it will recover its shape and superelastic properties upon heating over the Af temperature. Moreover, a hybrid martensite microstructure (like the HyFlex® CM™ controlled-memory files) is more likely to have more favorable fatigue resistance than an austenitic microstructure. At the same stress intensity level, the fatigue crack propagation speed of austenitic structures is much faster than that of martensite ones. A quantitative analysis based on the model of the fracture process zone showed that the martensite transformation in the shape memory nickel-titanium alloy caused a 47% increase in the apparent fracture toughness (Wang, 2007).
Very recently, controlled-memory thermo-mechanical processing was combined with an innovative machining procedure for the manufacturing of rotary nickel-titanium endodontic files. The procedure is called electrical discharge machining (EDM) and results in instruments of increased surface hardness cutting efficiency and extreme fatigue resistance. In the first paper published evaluating these files (Pirani, et al., 2015), spark-machined peculiar surface was mainly noticed, and low degradation was observed after multiple canal instrumentations. The authors also found high values of cyclic fatigue resistance and a safe in vitro use in severely curved canals. In agreement with these previews researchers, Pedulla, et al., 2015, reported higher values of fatigue resistance for EDM rotary files even when compared with reciprocating files made from M-Wire.
The extreme flexibility and fatigue resistance of these files combined with the lack of restoring force render them ideal to be used for the instrumentation of highly curved and complicated canals. Whenever a conventional superelastic nickel-titanium file is rotating inside a curved canal, it creates its own trajectory guided by the restoring force of the file and transporting the canal toward the outer apical curve (Elayouti, et al., 2011). The bigger the size or taper of the file used, the more dentin is removed from the outer apical curve, resulting in off-centered preparation at this level.
Leseberg and Montgomery (1991) studied canal transportation at the level of the curve and documented the distal (toward the midline) movement of the original canal. They showed that canal transportation is caused by a combination of forces resulting from the restoring force of the instrument that rotates around the clinical and proximal view curvatures. These forces produce a transportation vector distally and axially at this level. From their study, it would appear that for the middle third of a given curved canal, the greater the clinical and proximal view curvatures, the faster the transportation would progress toward the distal concavity of the root. The dynamics of apical and middle third transportation, as the result of the restoring force of the instrument and the degree of canal curvature, can be seen in Figure 3.

However, controlled-memory files have no restoring force after bending in body and room temperature. Whenever an instrument with controlled-memory characteristics is activated inside a curved canal, it moves passively inside the anatomy producing minimal forces of transportation. In highly curved canals, the lack of restoring force keeps the CM files rotating toward the outer canal wall at the fulcrum of the curvature (Figure 4).
Similar transportation dynamics with controlled memory were also demonstrated during the instrumentation of double-curved canals (Burroughs, et al., 2012). In simulated S-shaped canals, controlled-memory files produced more overall transportation compared to SAF and M-Wire instruments. Although the overall transportation was found bigger for no shape memory files, they always transported the double-curved canal toward the outer curves. This is very important in highly curved and double-curved canals because the initial dentinal thickness of human curved roots is always minimal at the convexity of the inner distal curves (danger zones) or the inner S-apical curves (Figure 5).

TCA instrumentation technique
Root canal instrumentation involves the use of hand- or engine-driven files to create sufficient space for irrigation and medication. The tactile feedback of the root canal anatomy felt by the operator during this procedure depends on various factors, including:
- the initial canal shape (round, oval, long oval, or flat canals)
- the canal length (the longer the canal, the more frictional resistance is expected)
- the canal taper (tapering discrepancy between a gauging instrument and the canal may cause false binding sensation)
- the canal curvature (curved canals can cause deflection of the instruments and increase frictional resistance)
- the canal content (fibrous or calcified canal content can create different degrees of frictional resistance)
- canal irregularities (attached pulp stones, denticles, and reparative dentin can create convexities on root canal walls)
- the type of instrument used (rigidity, flexibility, tapering, and restoring force can alter the frictional feedback) (Jou, et al., 2004)
For a given root canal and a given file, the operator’s tactile feedback during the instrumentation procedure differs according to the kinematics of the file used. Passively inserted files (non-activated) give a tactile sensation that is determined by the frictional resistance generated when the file engages the dentinal walls. The tactile sensation with an activated file (rotating or reciprocating), however, as the result of cutting, can more accurately be determined by the ability of the file to resist advancement around curvatures while in action (McSpadden, 2007).
Keeping in mind the complexity of root canal systems and the need to minimize file engagement during instrumentation, a novel approach was developed and named as the TCA instrumentation technique. The TCA technique can be defined as the activation of a motionless engine-driven file only after it becomes fully engaged inside a patent canal (Chaniotis, Filippatos, 2015). TCA utilizes file activation only after maximum engagement of the flutes is reached and a tactile feedback of the anatomy is felt. Inserting files passively (non-activated) inside the root canals and using controlled-memory instruments that can be pre-curved before file insertion is suggested to be advantageous, especially when complicated canal systems are encountered and limited mouth opening hinders canal negotiation and visualization. The TCA technique can be divided into in-stroke and out-stroke components.
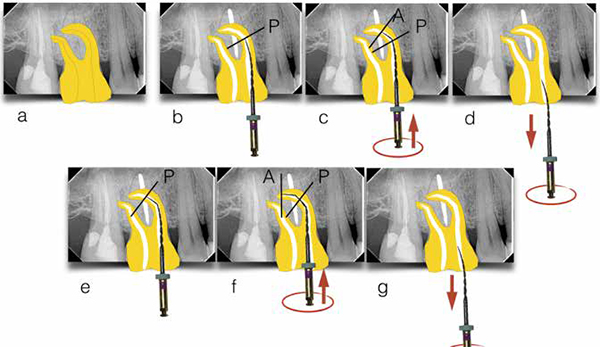
After accessing the pulp chamber and locating the canal orifices, technical patency to length is confirmed (Figure 6A). The first file to be used is mounted on the handpiece of an endodontic motor and inserted passively inside the canal until maximum frictional resistance (Figure 6B – point B). The file is activated and pushed apically (in-stroke) until the activated file resists further advancement (Figure 6C – point A) and withdrawn from the canal (Figure 6D). After file withdrawal, the file is inactivated; the flutes are cleaned and checked for any possible deformations. Irrigation and patency confirmation follows. The second time that the same file will be inserted passively inside the same canal, it will reach deeper inside the anatomy (Figure 6E – point P). Activating the file again the same way will guide the file even more apically closer to length (Figure 6F – point A). The work to be done by this file is completed when the file can reach working length without having to activate it and is then withdrawn (Figure 6G).
Instrumentation to larger apical preparations is achieved the same way until the desired apical instrumentation width is achieved. TCA technique aims to minimize the time of engagement with an activated file by using file activation only when needed for advancement. With this instrumentation technique, most of the anatomical root canal variations can be enlarged safely to the desired instrumentation size, irrespective of the degree and complexity of canal curvatures, by maintaining a tactile sensation of the anatomy throughout the whole procedure. For dilacerated canals, the controlled-memory files can be pre-curved in order to negotiate passively below the fulcrum of the abrupt curvature, activated at the point of maximum engagement and withdrawn from the canal (out-stroke) instead of advancing them deeper.
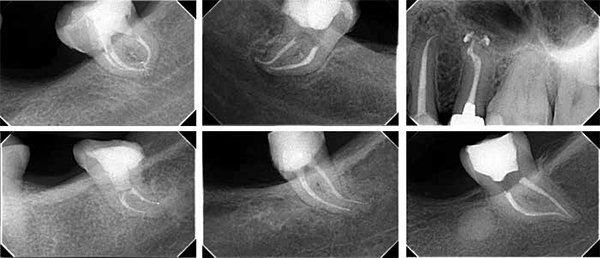
The next time that the same file will be inserted passively inside the dilacerated canal, engagement of the flutes will be felt more apically. The file is activated the same way and withdrawn from the canal. This way, engine-driven files can negotiate the apical third of dilacerated canals safely by maintaining a tactile sensation of the anatomy throughout the whole instrumentation procedure (Chaniotis, Filippatos, 2015). Challenging cases of extreme canal curvature that were managed with TCA instrumentation technique with controlled-memory files can be seen in Figure 7.
Controlled-memory file sequencing
The file sequencing during endodontic instrumentation is directly related to the anatomical challenge encountered. In a roentgenographic investigation of frequency and degree of canal curvatures in human permanent teeth, 84% of the root canals were found curved, and 17.5% of them presented a second curvature and were classified as S-shaped root canals (Schäfer, et al., 2002). From all the curved canals, 75% were found to have a small curvature of less than 27°, 15% a medium curvature ranging from 27° to 35°, and 10% a severe curvature of more than 35°.
Usually, patent root canals with a curvature of less than 27º are considered easy and straightforward cases for most instrumentation systems available today, and they pose no significant problems to the clinician. The enhanced physical properties of controlled- memory files manufactured with the electrical discharge machining procedure makes it possible to shape a canal with the use of a single file in 360º continuous movement. Most of these cases can be shaped quite quickly, effectively, and safely by using a single HyFlex™ EDM file 25 (Coltene) with the TCA technique.
The one EDM HyFlex file has a tip size of 25 with a 0.08 taper. The taper is a constant 0.08 in the apical 4 mm of the instruments but reduces progressively up to 0.04 in the coronal portion of the instrument. The file has three different cross-sectional areas over the entire length of the working part (rectangular in the apical part and two different trapezoidal cross sections in the middle and coronal part of the instrument) to increase its fracture resistance and cutting efficiency (Pedulla, et al., 2015). Whenever larger apical preparations are required, three finishing HyFlex EDM files of constant taper can be used (40/04, 50/03, and 60/02).
Constricted and obliterated canals, thin and long roots, curved canals of more than 27º, and S-shaped canals with smaller than 5 mm radius of curvature are considered challenging for all instrumentation systems available nowadays. With controlled-memory files, these cases are more effectively, safely, and predictably enlarged with the soft, ductile, and fatigue-resistant HyFlex CM files by following a simple standardized protocol and TCA technique.
After flaring with the 25/08 HyFlex CM flaring file and glide path creation to 10/02 hand file, HyFlex CM files can be used with the TCA technique in a standardized simple protocol of 15/04-20/04-25/04-30/04 and 35/04. This sequence is easy to remember and can work effectively and safely even in the most challenging situations of root canal instrumentation.
The final enlargement will be dictated by the initial anatomy of each root. For glide path creation, the EDM 10/05 glide path file can also be used after flaring and initial canal scouting. In multi-canal teeth, easier canals can be instrumented with a single EDM file 25, and the complicated ones with the aforementioned CM file sequence. In this way, safe and predictable instrumentation to adequate apical preparation size that respects canal anatomy can be achieved.
Conclusions
- Controlled-memory files have no shape memory effect, increased flexibility, and fatigue resistance. As a result, they move passively inside the highly curved or double-curved canals guided only by the anatomy and not by the restoring force of other files.
- The TCA instrumentation technique minimizes the time that the files are under engagement inside challenging canals and results in maintaining a continuous tactile feedback of the anatomy throughout the whole instrumentation procedure.
- Although the TCA technique can be used with all instrumentation systems available (rotary or reciprocation), controlled-memory systems are the only ones where the files can be pre-bent for easier negotiation of challenging cases (abrupt curvatures, ledges, and limited mouth-opening patients).
- EDM files with controlled-memory characteristics have increased cutting efficiency and fatigue resistance. This makes it feasible to use a single file instrumentation protocol for approximately 75% of human root canals.
References
- AAE Glossary of Endodontic Terms. 8th edition. 2012.
- Baumann MA. Nickel-titanium: options and challenges. Dental Clin North Am. 2004 ;48(1): 55-67.
- Boutsioukis C, Gogos C, Verhaagen B, Versluis M, Kastrinakis E, Van der Sluis LW. The effect of apical preparation size on irrigant flow in root canals evaluated using an unsteady Computational Fluid Dynamics model. Int Endo J. 2010;43(10): 874-881.
- Burroughs JR, Bergeron BE, Roberts MD, Hagan JL, Himel VT. Shaping ability of three nickel-titanium endodontic file systems in simulated S-shaped root canals. J Endo. 2012;38(12):1618-1621.
- Burroughs JR, Bergeron BE, Roberts MD, Hagan JL, Himel VT. A case report. Int Endod J. In press.
- HyFlex® CM™ [brochure]. Cuyahoga Falls, Ohio: Coltene/Whaledent; 2012.
- Elayouti A, Dima E, Judenhofer MS, Löst C, Pichler BJ. Increased apical enlargement contributes to excessive dentin removal in curved root canals: a stepwise microcomputed tomography study. J Endod. 2011;37(11):1580-1584.
- Estrela C, Bueno MR, Sousa-Neto MD, Pechora JD. Method for determination of root curvature radius using cone-beam computed tomography images. Bras Dent J. 2008;19(2):114-118.
- Joe Y-T, Karabucak B, Levin J, Liu D. Endodontic instrumentation width: current concepts and techniques. Dent Clin North Am. 2004;48(1):323-335.
- Leseberg DA, Montgomery S. The effects of Canal Master, Flex-R, and K-Flex instrumentation on root canal configuration. J Endod. 1991;17(2):59-65.
- Günday M, Sazak H, Garip Y. A comparative study of three different root canal curvature measurement techniques and measuring the canal access angle in curved canals. J Endod. 2005;31(11): 796-798.
- Hulsmann M, Peters O, Dummer P. Mechanical preparation of root canals: shaping goals, techniques and means. Endod Topics. 2005;10(1):30-76.
- McSpadden JT. Mastering endodontic instrumentation. Chattanooga, TN: Cloudland Institute; 2007.
- Nagy CD, Szabó J, Szabó J. A mathematically based classification of root canal curvatures on natural human teeth. J Endod.1995;21(11):557-560.
- Peters OA. Current challenges and concepts in the preparation of root canal systems: a review. J Endod. 2004;30(8):559-567.
- Plotino G, Grande NM, Mazza C, Petrovic S, Testarelli L, Gambarini G. Influence of size and taper of artificial canals on the trajectory of NiTi rotary instruments in cyclic fatigue studies. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010;109(1):e60-e66.
- Pirani C, Iacono F, Generali L, et al. HyFlex EDM: superficial features, metallurgical analysis and fatigue resistance of innovative electro discharge machined NiTi rotary instruments. Int Endod J. 2015;49(5):483-493.
- Pedulla E, Lo Savio F, Boninelli S, et al. Torsional and cyclic fatigue resistance of a new nickel-titanium instrument manufactured by electrical discharge machining. J Endod. 2016;42(1):156-159.
- Pruett JP, Clement DJ, Carnes DL Jr. Cyclic fatigue testing of nickel-titanium endodontic instruments. J Endod. 1997; 23(2):77-85.
- Roane JB, Sabala CL, Duncanson MG Jr. The “balanced force” concept for instrumentation of curved canals. J Endod. 1985;11(5):203-211.
- Schäfer E, Diez C, Hoppe W, Tepel J 2002 Roentgenographic investigation of frequency and degree of canal curvatures in human permanent teeth. J Endod. 2002;28(3):211-216.
- Shen Y, Qian W, Abtin H, Gao Y, Haapasalo M. 2011 Fatigue testing of controlled memory wire nickel-titanium rotary instruments. J Endod. 2011;37(7):97-1001.
- Schilder H. Cleaning and shaping the root canal. Dent Clin North Am. 1974;18(2):269-296.
- Schneider SW. A comparison of canal preparations in straight and curved root canals. Oral Surg Oral Med Oral Patho. 1971;32(2):271-275.
- Walia HM, Brantley WA, Gerstein H. An initial investigation of bending and torsional properties of Nitinol root canal files. J Endod. 1988;14(7):346-351.
- Wang GZ. Effect of martensite transformation on fracture behavior of shape memory alloy NiTi in a notched specimen. Int J Fract. 2007;146(7):93-104.
Stay Relevant With Endodontic Practice US
Join our email list for CE courses and webinars, articles and more..
