Drs. Fernando Muñoz Ayón, Jorge Paredes Vieyra, and Victor Manuel de la Torre Martínez demonstrate a nonsurgical endodontic retreatment of an extensive periapical lesion of endodontic origin with Vitapex®
 Apical periodontitis and its accompanying periapical bone resorption are inflam-matory disorders of periradicular tissues caused by persistent microbial infection within the root canal system of the affected tooth (Safavi and Nichols, 1993). Incessant apical periodontitis after root canal treatment often portrays a more complex scenario than primary apical periodontitis (Nair, 2006).
Apical periodontitis and its accompanying periapical bone resorption are inflam-matory disorders of periradicular tissues caused by persistent microbial infection within the root canal system of the affected tooth (Safavi and Nichols, 1993). Incessant apical periodontitis after root canal treatment often portrays a more complex scenario than primary apical periodontitis (Nair, 2006).
The most common causes for failure in endodontics include the inability to eradicate bacteria from the root canal system after treatment, reinfection of the root canal by coronal leakage (Haapasalo, et al., 2007), extraradicular infection, foreign body reaction, and true cysts (Cohen, Hargreaves, and Berman, 2011). In such cases where primary endodontic therapy does not succeed, a nonsurgical endodontic retreatment approach is the best option.
The main difference between treating primary endodontic disease versus post-treatment disease is the need to regain access to the apical third of the root canal previously treated. Once this is achieved, all of the principles of endodontic therapy apply to the completion of the retreatment case (Cohen, Hargreaves, and Berman, 2011), including cleaning, shaping, and inter-appointment dressings. The most widely used intracanal medication to date continues to be calcium hydroxide Ca(OH)2. Its antimicrobial mechanism and high pH (12.5) provide an environment where few microorganisms are able to survive. Another drug used with high antibacterial activity is iodoform (CHI3), which has been used successfully as a medicament and filling paste for many years (Pallota, et al., 2010). Vitapex® (Neo Dental International, Inc.) is a commercial Ca(OH)2 paste used as root canal dressing in primary and permanent teeth; it also contains CHI3 and inhibits or kills the pathogen in the root canal; furthermore, it can promote bone repairment and regeneration, as shown by Xia and colleagues (2013).
Although very effective eliminating bacteria inside the canal, removal of these Ca(OH)2 pastes is often difficult. Passive ultrasonic irrigation (PUI) has proven to be effective in Ca(OH)2 removal (63.3%) from the root canal wall due to its cavitation and microstreaming effect on NaOCl compared with syringe delivery. However, whether PUI can effectively remove Ca(OH)2 from the root canal wall is not well-known (van der Sluis, Wu, and Wesselink, 2007).
During root canal treatment, Ca(OH)2 pastes might sometimes unintentionally escape through the apex of the tooth. The deliberate placement of Ca(OH)2 beyond the confines of the root canal in the presence of large and chronic periapical lesions has been advocated. Some speculate that this favors periapical healing and encourages osseous repair. Such deliberate overextension is not, however, widely advocated (Orocoglu and Cobankara, 2008).
Case report
A 42-year-old female patient was referred to our office for treatment of maxillary left lateral incisor tooth. The reason for consultation was completion of root canal therapy, which had been left unfinished 2 to 3 years to date.
 Upon questioning, the patient reported mild pain with the presence of a sinus 3 months previously. The patient also reported pain on mastication 3 days prior to this appointment, and clinical examination confirmed the presence of purulent exudate on palpation at the gingival margin, as well as a palatal groove and composite filling on access cavity (Figure 1). The right lateral incisor was slightly sensitive to percussion and palpation. Radiographic evaluation (Schick CDR, Schick Technologies) demonstrated a very acceptable endodontic treatment accompanied with a radiolucent lesion approximately 10 mm in diameter around the apex (Figure 2).
Upon questioning, the patient reported mild pain with the presence of a sinus 3 months previously. The patient also reported pain on mastication 3 days prior to this appointment, and clinical examination confirmed the presence of purulent exudate on palpation at the gingival margin, as well as a palatal groove and composite filling on access cavity (Figure 1). The right lateral incisor was slightly sensitive to percussion and palpation. Radiographic evaluation (Schick CDR, Schick Technologies) demonstrated a very acceptable endodontic treatment accompanied with a radiolucent lesion approximately 10 mm in diameter around the apex (Figure 2).
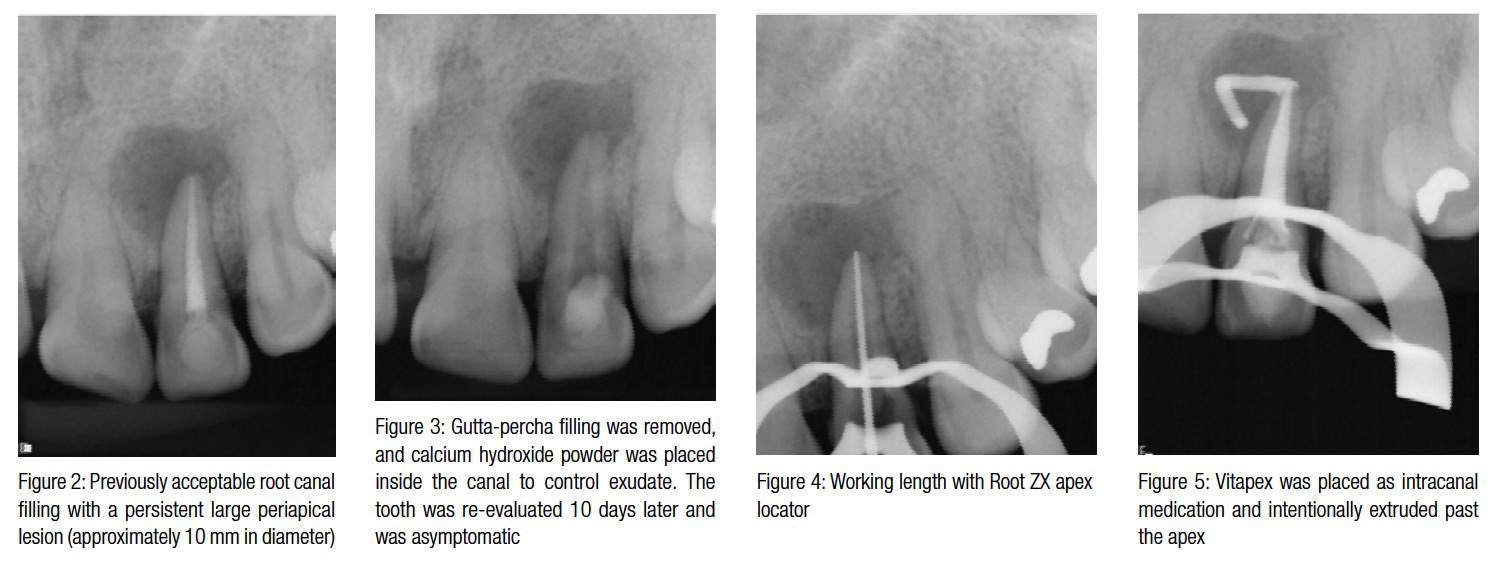

Nonsurgical retreatment approach was planned, and informed consent was given and signed by the patient. Treatment was performed without local anesthesia and with rubber dam in place. The access cavity was prepared with carbide bur No. 2 (Mani®, Inc.) and Endo-Z™ (Dentsply International). Removal of gutta percha was attempted via ProTaper® Universal Retreatment files (Dentsply Tulsa Dental Specialties). Once inside the canal, a calcium hydroxide paste was found, removed, and 2.5% sodium hypochlorite irrigating solution was administered as final rinse. Canal was dried with sterile paper points (Coltène Whaledent Group, Hygenic®), and calcium hydroxide powder (Sultan Healthcare Inc.) was placed into the canal to control the exudate. The tooth was temporarily restored with intermediate restorative material (IRM® Caulk; Dentsply).
 Clinical evaluation was performed after 10 days (Figure 3). The tooth was asymptomatic and isolated in the same manner as that described in the previous appointment. Working length was then determined by an electronic apex locator (Root ZX®, J. Morita) with a No. 45 K-file (Mani, Inc.) (Figure 4).
Clinical evaluation was performed after 10 days (Figure 3). The tooth was asymptomatic and isolated in the same manner as that described in the previous appointment. Working length was then determined by an electronic apex locator (Root ZX®, J. Morita) with a No. 45 K-file (Mani, Inc.) (Figure 4).
During this appointment 2.5% NaOCl was administered; the canal was then dried in the same manner as previous appointment, and Vitapex was placed as intracanal dressing and intentionally placed in the periradicular area through the apex (Figure 5). A cotton pellet was placed in the pulp chamber, and the tooth was temporarily restored with intermediate restorative material (IRM Caulk; Dentsply).
The patient lost all contact with our practice and returned 17 months later with mild pain and a cast post and metal porcelain crown in the unfinished root canal treatment. After removal of cast post and crown, the canal preparation was accomplished with F4 and F5 ProTaper Universal files (Figures 6-7). Canals were obturated by means of the lateral condensation technique and Sealapex™ sealer. After 1 month (Figure 8), the patient was asymptomatic, and mild healing of the perirapical lesion was observed, even though no permanent crown had been placed.
The patient lost contact once again, but 1 year later returned, asymptomatic, and the tooth and periapical tissues appeared to be healing correctly with total repair and proper function of the tooth (Figure 9).
Discussion
From a microbial perspective, after pulp necrosis, infection of the root canal system occurs. Microorganisms then inhabit the oral cavity like bacteria, and fungi invoke a protective inflammatory response in the periradicular tissues. However, when host defense systems cannot enter the necrotic root canal and eliminate the invading microbes, the inflammatory process results in the formation of abscesses, granulomas, and/or periapical cysts, as shown by Love and Firth (2009) and Soares and colleagues (2008).
Such lesions can only be detected radiographically when alveolar bone loss has been accompanied by cortical bone involvement during lesion development (Soares, et al., 2008; Arslan, et al., 2012). The mean diameter of apical lesions ranges from 5 mm-8 mm; lesions of 10 mm or more are considered granulomas or apical cysts (Soares, et al., 2008; Soares, et al., 2006). Even though the incidence of radicular cysts is approximately 15% of all periapical lesions, healing of all apical periodontitis ranges from 80%–95% after root canal treatment, which alone suggest that cysts may heal without surgery (Love and Firth, 2009; Soares, et al., 2008; Arslan, et al., 2012; Soares, et al., 2006). Therefore, management of large periapical lesions by nonsurgical procedures should always be considered.
Because surgical procedures come with many drawbacks (for example, possible damage to adjacent vital teeth and anatomic structures in the vicinity, pain, and dis-comfort), its use is limited in the management of periapical lesions, as shown by Thomas, Dhanapal, and Simon (2012). However, non-surgical endodontic treatment focuses on the removal of all bacteria and their byproducts from the root canal system (Tavares, et al., 2012; Torabinejad, et al., 2005); adherence to these treatment objectives should result in maintaining normal radiographic and clinical conditions in teeth with and without pre-
operative periradicular lesions (Torabinejad, et al., 2005). Based on available studies that offer the best evidence, it appears 92%-98% of teeth without periapical lesions remain free of disease after root canal therapy, and 74%-86% of teeth with apical lesions completely heal after initial treatment or retreatment. In addition, similar data shows that 91%-97% of teeth that have had root canal treatment remain functional over time (Torabinejad, et al., 2005). Still, in some cases, a bone lesion takes a considerable time to heal, which means that conclusions about outcome are sometimes uncertain. Apical periodontitis may also heal with fibrous tissue rather than bone. Such scar tissue healing is usually thought to have a typical radiographic appearance and is mostly seen after endodontic surgical procedures (Peterson, et al., 2012).
Broon and colleagues showed that the inability to achieve infection control after root canal treatment can result in a chronic inflammatory process (2007). For such cases, the use of intracanal medication is widely advocated. Various studies found that the use of Ca(OH)2 dressing for 1 to 4 weeks efficiently removed bacteria from the root canals (Estrela, et al., 2001; Zmener, Pameijer, and Banegas, 2007; Han, Park, and Yoon, 2001).
Although the use of these Ca(OH)2 pastes is highly effective, its removal from the root canal is often a difficult task. Removal of pastes like Vitapex is often done by instrumentation of the root canal with the master apical file combined with abundant irrigation of both NaOCl and EDTA.
In a recent study, passive ultrasonic irrigation (PUI) proves to be effective in Ca(OH)2 removal (63.3%) from the root canal wall due to its cavitation and microstreaming effect on NaOCl compared with syringe delivery (van der Sluis, Wu, and Wesselink, 2007). In the present case, the extrusion of Vitapex through the apex possibly delayed the apical healing, but did not prevent it. Our case results agree with findings by Arslan, Broon, Soares, Thomas, van der Sluis, and Xia (2012; 2007; 2006; 2012; 2007; 2013), as the large periapical lesion was retreated without surgical intervention, the intentional extrusion of Vitapex promoted the periapical healing, and PUI served as an excellent Ca(OH)2 paste (Vitapex) remover from the root canal as well as the diffusion of NaOCl into the dentinal tubules.
Conclusion
When endodontic therapy cannot eliminate bacteria from the canal, and large periapical lesions develop on previously treated teeth, nonsurgical root canal retreatment should always be considered before a surgical approach. In the present case, a nonsurgical approach in combination with calcium hydroxide/iodoform paste as an intracanal medicament contributed effectively in limited healing of the periapical lesion at 1 month and nearly fully repaired at 1 year. This confirms that large periapical lesions can respond positively to nonsurgical retreatment.
Acknowledgment
We thank Professor Dr. Michael Hülsmann (Göttingen, Germany) for his valuable assistance in reviewing this manuscript.
References
- Arslan H, Karataş E, Barutcugil Ç, Topçuoğlu HS, Aladağ H. Treatment of large periapical lesions without surgical approach: report of three cases. Int Dent Res. 2012;2(1):17-22.
- Broon NJ, Bortoluzzi EA, Bramante CM. Repair of large periapical radiolucent lesions of endodontic origin without surgical treatment. Aust Endod J. 2007;33(1): 36-41.
- Estrela C, Bammann LL, Pimenta FC, Pécora JD. Control of microorganisms in vitro by calcium hydroxide pastes. Int Endod J. 2001;34(5):341-345.
- Haapasalo M, Qian W, Portenier I, Waltimo T. Effects of dentin on the antimicrobial properties of endodontic medicaments. J Endod. 2007;33(8):917-925.
- Han GY, Park SH, Yoon TC. Antimicrobial activity of Ca(OH)2 containing pastes with Enterococcus faecalis in vitro. J Endod. 2001;27(5):328-332.
- Love RM, Firth N. Histopathological profile of surgically removed persistent periapical radiolucent lesions of endodontic origin. Int Endod J. 2009;42(3):198-202
- Nair PN. On the causes of persistent apical periodontitis: a review. Int Endod J. 2006;39(4):249-281.
- Orucoglu H, Cobankara FK. Effect of unintentionally extruded calcium hydroxide paste including barium sulfate as radiopaquing agent in treatment of teeth with periapical lesions: report of a case. J Endod. 2008;34(7):888-891.
- Pak JG, Fayazi S, White SN. Prevalence of periapical radiolucency and root canal treatment: a systematic review of cross-sectional studies. J Endod. 2012;38(9):1170-1176.
- Pallotta RC, de Lima Machado ME, dos Reis NS, Rosa Martins GH, Nabeshima CK. Tissue inflammatory response to implantation of calcium hydroxide and iodoform in the back of rats. Rev Odont C. 2010;25(1):59-64.
- Petersson A, Axelsson S, Davidson T, Frisk F, Hakeberg M, Kvist T, Norlund A, Mejáre I, Portenier I, Sandberg H, Tranæus S, Bergenholtz G. Radiological diagnosis of periapical bone tissue lesions in endodontics: a systematic review. Int Endod J. 2012;45(9):783-801.
- Roda RS, Gettleman BH. Nonsurgical Retreatment. In: Cohen S, Hargreaves KM, Berman LH eds. Pathways of the Pulp. 10th ed. St. Louis, MO: Mosby, Inc; 2011: 890-952.
- Safavi KE, Nichols FC. Effect of calcium hydroxide on bacterial lipopolysaccharide. J Endod. 1993;19(2):76-78.
- Soares J, Santos S, Silveira F, Nunes E. Nonsurgical treatment of extensive cyst-like periapical lesion of endodontic origin. Int Endod J. 2006;39(7):566–575.
- Soares JA, Brito-Júnior M, Silveira FF, Nunes E, Santos SM. Favorable response of an extensive periapical lesion to root canal treatment. J Oral Sci. 2008;50(1):107-111.
- Tavares WL, de Brito LC, Henriques LC, Teles FR, Teles RP, Vieira LQ, Ribeiro Sobrinho AP. (2012) Effects of calcium hydroxide on cytokine expression in endodontic infections. J Endod. 2012;38(10):1368-1371.
- Thomas K, Dhanapal PT, Simon EP. Management of large periapical cystic lesion by aspiration and nonsurgical endodontic therapy using calcium hydroxide paste. J Contemp Dent Pract. 2012;13(6):897-901.
- Torabinejad M, Kutsenko D, Machnick TK, Ismail A, Newton CW. Levels of evidence for the outcome of nonsurgical endodontic treatment. J Endod. 2005;31(9): 637-646.
- Van der Sluis LW, Wu MK, Wesselink PR. The evaluation of removal of calcium hydroxide paste from an artificial standardized groove in the apical root canal using different irrigation methodologies. Int Endod J. 2007;40(1): 52-57.
- Xia X, Man Z, Jin H, Du R, Sun W, Wang X. Vitapex can promote the expression of BMP-2 during the bone regeneration of periapical lesions in rats. J Indian Soc Pedod Prev Dent. 2013;31(4):249-253.
- Zmener O, Pameijer CH, Banegas G. An in vitro study of the pH of three calcium hydroxide dressing materials. Dent Traumatol. 2007;23(1):21-25.
Stay Relevant With Endodontic Practice US
Join our email list for CE courses and webinars, articles and more..
