Dr. Albert (Ace) Goerig discusses the benefits of 3D imaging to the diagnostic process
As a practicing endodontist for over 40 years, I’m always looking for new innovations to keep me excited about endodontics and expand my technical and diagnostic skills. In 2008, I purchased my first cone beam computed tomography (CBCT) unit and used it occasionally. Once I attended Dr. Marty Levin’s 2-day course on how to use the CBCT in endodontics, I then fully understood its capabilities and began using it many times during the day. I would say this technology is one of the top four most important endodontic developments in the past 30 years — with the others being motorized engine files, microscopes, and digital radiography. Many of our referring dentists are looking for a reason to refer their patients to our office, and this is the big one. Here is a list of some advantages of this technology that I share with my referring doctors.
The CBCT helps us determine tooth morphology, including location and number of canals, pulp chamber size and degree of calcification, root structure, direction and curvature, root tip extruding outside the cortical plate, fractures, iatrogenic defects, and the extent of dental caries. CBCT also identifies locations of anatomical landmarks such as the mandibular canal and sinus in relationship to the tooth. When assessing dental trauma, it is incredible in detecting horizontal root fractures and cortical bone fractures. CBCT is essential in determining the degree and extent of internal and external resorption and determining if an extraction would be the best treatment option.
With a difficult diagnostic case where the periapical lesion does not show up on a normal radiograph, it usually becomes evident with CBCT. Here is an example of a patient with severe pain, no swelling, and all teeth nonresponsive to hot, cold, or percussion. Once the scan was taken, the diagnosis was obvious — the tooth required treatment of tooth No. 30. It is amazing how many other asymptomatic teeth with radiolucencies are found on the scan adjacent to teeth being treated.
Finding the size and locations of periapical lesions and proximity to anatomic landmarks such as the mandibular canal is imperative, especially if periapical surgery is being considered. This is especially helpful in routine root canal treatment of lower second molars, making sure not to overfill into the mandibular canal.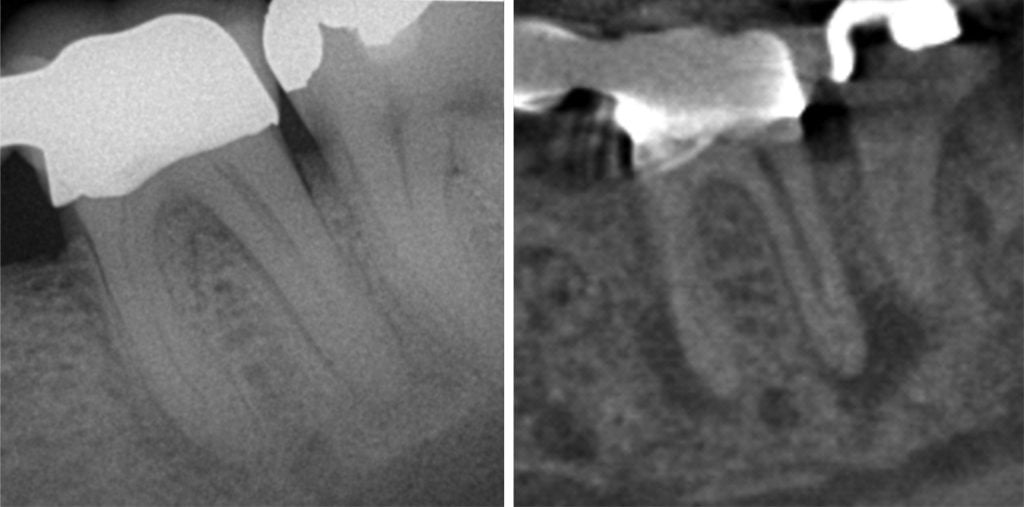
Figure 1
How often in the past have we retreated poorly filled root canals and determined later the infection was due to a vertical root fracture? Here is a case I treated over 20 years ago, and the patient complained of tenderness while chewing. Even though it’s not readily visible on the standard radiograph, the CBCT showed extensive bone loss all the way down the mesial lingual root, indicating a vertical root fracture and confirmed upon extraction.
Anytime I believe there is complex dental anatomy, I take a scan. There is a standing order among my team members to take a scan on all upper molars before I enter the room. This helps me determine the exact location and presence of the second mesial buccal canal. This not only saves unnecessary removal of root structure, but also reduces reduces patient chair time. About 5% of the time, the palatal and distal buccal roots of maxillary molars connect all the way to the apex. Many of these can fail unless you find the extra canals in the root. Most retreatments of the maxillary molars are due to the missed MB2 canal.
CBCT scanning has elevated the standard of care of endodontics. This will become one of the main reasons why doctors refer to us. CBCT improves our diagnostic accuracy; increases speed of treatment; and improves productivity, patient satisfaction, and patient outcomes. It’s fun to have such a powerful tool that brings so much value to the diagnostic aspect of the practice!
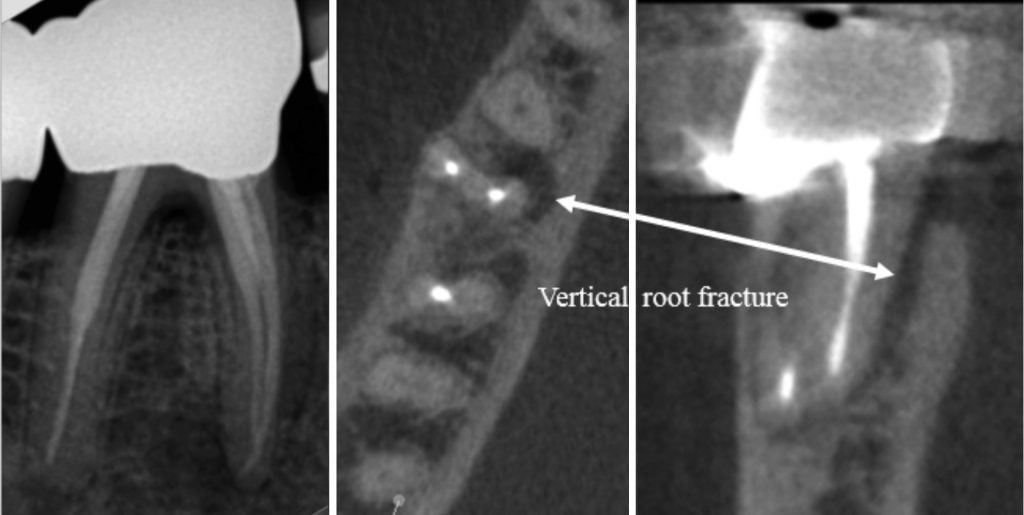
Figure 2

Figure 3
 Albert (Ace) Goerig, DDS, MS, is a nationally known speaker who has lectured extensively in his field of endodontics and dental practice management to dentists throughout the United States, Canada, and abroad. He has authored over 60 articles and is a contributing author to the following textbooks: Pathways of the Pulp, Ingle’s Endodontics, and Practical Endodontics. Dr. Goerig is a Diplomate of the American Board of Endodontics and a Fellow of both the American and International College of Dentists. He has been involved in teaching both endodontics and general dentistry residents for many years. He is in private dental practice in Olympia, Washington, specializing in endodontics. In 1996, he co-founded Endodontic Practice Mastery to teach endodontists the business of dentistry while helping them to love their practice. Since then he has personally coached over 22% of all endodontists and their teams in the U.S. and Canada. He is also the co-author of Time and Money: Your Guide to Financial Freedom. Dr. Goerig and his wife, Nancy, were married in 1969 and have five children. He has many hobbies, including fishing, scuba diving, skiing, and travel.
Albert (Ace) Goerig, DDS, MS, is a nationally known speaker who has lectured extensively in his field of endodontics and dental practice management to dentists throughout the United States, Canada, and abroad. He has authored over 60 articles and is a contributing author to the following textbooks: Pathways of the Pulp, Ingle’s Endodontics, and Practical Endodontics. Dr. Goerig is a Diplomate of the American Board of Endodontics and a Fellow of both the American and International College of Dentists. He has been involved in teaching both endodontics and general dentistry residents for many years. He is in private dental practice in Olympia, Washington, specializing in endodontics. In 1996, he co-founded Endodontic Practice Mastery to teach endodontists the business of dentistry while helping them to love their practice. Since then he has personally coached over 22% of all endodontists and their teams in the U.S. and Canada. He is also the co-author of Time and Money: Your Guide to Financial Freedom. Dr. Goerig and his wife, Nancy, were married in 1969 and have five children. He has many hobbies, including fishing, scuba diving, skiing, and travel.
Stay Relevant With Endodontic Practice US
Join our email list for CE courses and webinars, articles and more..
