Dr. Barry Musikant examines the techniques and solutions of two instrumentation systems, using the literature and illustrated cases
It’s not a contradiction until you realize it is. Greater tapered rotary nickel-titanium (NiTi) shaping has produced a mechanical standard for cleansing and shaping canals.
It is only recently that research is documenting the weakening of the root via the removal of excess dentin, particularly in the mesiodistal plane due to the use of greater tapered instruments and the creation of dentinal microcracks in the process of shaping the canals with instruments in rotation, whether continuous or interrupted.
[userloggedin]
1-24
Dentinal microcracks should come as no surprise given the long and detailed documentation of metallic defects and frank separations that occur in the instruments. One is simply a reflection of the other following Newton’s laws of opposite and equal effects — that removal of excess dentin and the propensity to create microcracks where the dentin is thinnest and most subject to stresses is worth pondering. Rotational instrumentation combined with greater tapered instruments needlessly first inflicts a weakening of the root structure followed by damage to the integrity of the remaining dentin.
To date, an answer to these “side effects” has not been required because dentists were not aware that they occurred. As this information is dispersed more widely, one response is a form of rationalization that admits to the problem but quickly states that the advantages of these systems outweigh the disadvantages.
The basis of this defense is to maintain the status quo, support rotating greater tapered shaping in its present mode or, at most, make some minor changes in technique.
Perhaps the rationalizations stem from an apparent lack of alternatives. While this possibility might indeed be used, the same research that has illuminated greater tapered rotating instrumentation has also described techniques that neither lead to excess removal of dentin nor the introduction of dentinal microcracks, with the added benefit that instruments not inducing dentinal defects will themselves not be subject to separation.
Present conflicts
The answers to the present conflicts associated with “modern” endodontic techniques reside in the alternatives that deserve much further elaboration. Even prior to the use of greater tapered rotating instrumentation, creating a glide path with K-files has often proved problematic. The K-file instrument (Figure 1) designed with 30 predominantly horizontal flutes along its 16 mm of working length is known to frequently impact debris in the apical third, resulting in loss of length and the potential for canal distortion as the dentist attempts to reclaim that length.
In fact, a combination of poor results tied to major bouts of hand fatigue were a major impetus for the creation of greater tapered NiTi instrumentation. Typically, a dentist does not separate the glide path made with the manual use of K-files from the subsequent use of greater tapered NiTi instrumentation.
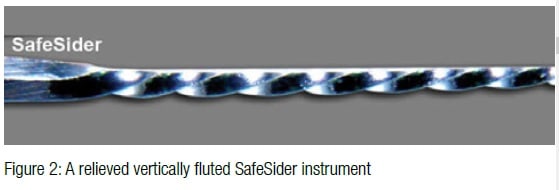
Yet, if we wish to enhance our effectiveness, relieved vertically fluted reamers (SafeSiders® [Essential Dental Systems], Figure 2) must substitute for K-files at the earliest stages of glide path creation. These reamers, designed with half the number of flutes along the same 16 mm of working length, have a flute orientation twice as vertical as those on a K-file. Unlike K-files that are all used manually, only the first and thinnest modified reamer required to negotiate to length is used manually. Once at the apex, the reamer is attached to a 30º reciprocating handpiece (Figure 3) oscillating at 3,000-4,000 cycles per minute. The vertical flutes on the reamer immediately shave dentin away with the first clockwise stroke. Having half the number of flutes to start with, the relieved reamers engage the dentin far less than the 30 flutes on a K-file, consequently encountering far less resistance to full apical negotiation. Oscillating at 3,000-4,000 cycles per minute, these instruments quickly enlarge the canal space, so the next instrument reaches the apex with minimal resistance.
The vertical flute orientation gives these instruments the ability to glide through any debris present rather than impacting it apically. A cutting tip limited to a 30º-45º arc of motion will pierce rather than impact tissue, again reducing the incidence of loss of length so common with K-files.
Using all the instruments in the 30º reciprocating handpiece eliminates hand fatigue and virtually eliminates the chances of instrument separation. Remember that an instrument not vulnerable to breakage is compatible in shaping canals without inducing dentinal defects — 02 tapered relieved stainless steel reamers are remarkably flexible through a 15 or 20, far more than their K-file counterparts. Furthermore, a highly tortuous canal is first negotiated and then enlarged with the thinnest most flexible instrument required.
At these dimensions, stainless steel is more than flexible enough to negotiate and widen canals without distortion. What is less understood is that a thin stainless steel relieved reamer oscillating at 3,000-4,000 cycles per minute will enlarge the canal to a dimension significantly greater than itself. This must be true because an 08 tipped reamer will encounter minimal resistance after the canal has been shaped with an 06 tipped reamer that initially met significant resistance. We see this fact clinically every day we practice.



Two more important observations have been made. As each larger relieved reamer oscillates through the length of the canal, the pathway is being more clearly defined, allowing subsequent and slightly less flexible instruments to faithfully follow the increasing established pathway. Once the dentists are fully confident that the instruments will remain intact, they will apply them more vigorously against the buccal and lingual walls of lateral canals.
This is in sharp contrast to the use of greater tapered rotary systems where they are used most safely in a centered position with little potential to effectively shape and cleanse these lateral extensions.
Most pulpal anatomy is not conical in shape. It is most often highly oval and sheath-like being consistently thin in the mesiodistal plane (with the exception of palatal roots) and several times wider in the buccolingual plane. A system that encourages dentists to remain centered is not designed to handle these situations that are more the rule than the exception.
Endo systems
The use of modified reamers employed in the 30º-45º reciprocating handpiece virtually eliminates hand fatigue, dentinal microcracks, and separated instruments while creating a glide path in three dimensions far more quickly than the manual approach necessary with the use of K-files. With the glide path shaped to a 20, the final shaping in the majority of cases creates an apical preparation of 30, a dimension considered the minimum for effective irrigation and a maximum taper of 04. To go from the 20 preparation to a 30/04 preparation requires only two more instruments — the Tango-Endo® Shaper (30/02) and the Tango-Endo® Finisher (30/04) (Essential Dental Systems). These instruments, unlike the SafeSiders, are used in a latch-type reciprocating handpiece that also oscillates at 3,000-4,000 cycles per minute.
The Tango-Endo System has a flute design that is significantly more efficient in working the lateral extensions of canals as compared to the SafeSiders, something that is important when attempting to remove tissue ensconced in the thin isthmuses. For the dentist’s safety, the highly efficient Tango-Endo System was designed to be latch-type instruments used in the Tango-Endo reciprocating handpiece. If these instruments had a manual hand-type handle, which could be used manually, there would be a chance of extensive engagement and over-torquing the instrument in the canal.
The two systems — the SafeSiders, providing the glide path without hand fatigue, and the Tango-Endo System, providing a fully shaped canal that preserves dentin in the thinner mesiodistal plane — work synergistically to atraumatically shape canals in a way that reflects their original anatomy in larger form.
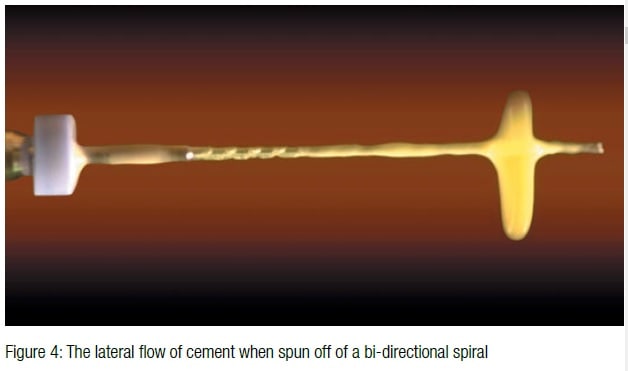
The canal is now ready to be obturated using a single Tango-Endo gutta-percha cone where the cone is thoroughly coated with epoxy resin cement (EZ-Fill®, Essential Dental Systems), and the canals are flooded with cement using the bi-directional spiral (Figure 4) as the applicator. Without question, the cement creates an effective seal. The gutta-percha point is nothing more than a carrier and a driver of the cement. The advantages of a passive single point room temperature technique include:
- Minimal stresses being transferred to the root the way they are when lateral, vertical, and thermal condensation techiques are used.
- No shrinkage. In fact, there is approximately 1.75% expansion as the room temperature cement and gutta percha warm to body temperature.
- A cement visocosity that flows better than the most thermoplasticized gutta percha available and then does not shrink.
A single point technique is obviously dependent upon the properties of the cement. EZ-Fill is an epoxy resin cement that has the following advantages:
- It is a polymer that is highly resistant to hydrolytic degradation.
- It is the most flowable of cements penetrating deeply into the dentinal tubules.
- It is highly radiopaque.
- It is highly antibacterial.
- It bonds chemically and physically to the both the gutta percha and the canal walls.
- If expressed over the apex, the macrophage digest it over 3 to 6 months.
Many root canal cements claim to be biocompatible and bone inductive, but their primary quality must be to provide a good long-term seal without producing prolonged irritation. Epoxy resins are a known quantity as a superior seal in endodontics with research going back over 60 years on their favorable properties.
Case presentations
I am presenting two cases that illustrate the ability of the two instrumentation systems working in concert to produce non-distorted shaping while also having the ability to penetrate the most calcified of cases. Note the small degree of taper that preserves tooth structure in the coronal third. The fillings are quite radiopaque because while thin in the mesiodistal plane, they extend the full length of the pulpal space in the wider buccolingual plane.
What we have succeeded in doing is enlarging the original canal anatomy in both planes and only to the degree necessary to remove the pulp tissue and a more or less uniform layer of circumferential dentin.
Aside from the initial thin reamer that was first negotiated to the apex, all instrumentation was done with the reciprocating handpiece oscillating at 3,000-4,000 cycles per minute, virtually removing all hand fatigue. Confined to a 30º-45º arc of motion, the instruments too are virtually free of separation, which in turn gives the dentist the confidence to use these instruments vigorously in the buccal and lingual planes.
By replacing rotation continuous or interrupted with 30º-45º reciprocation, using relieved reamers rather than K-files and limiting the maximum taper in most cases to an 04, we maintain the integrity of the instruments and the roots they are treating, reducing costs significantly while maintaining conditions that are more consistent with long term success. The goal is to remove enough tooth structure, but no more than that. We have shown the means to accomplish this goal in a timely and effective manner.
[/userloggedin]
[userloggedout][/userloggedout]
- Abou El Nasr HM, Abd El Kader KG. Dentinal damage and fracture resistance of oval roots prepared with single-file systems using different kinematics. J Endod. 2014;40(6):849-851.
- Adorno CG, Yoshioka T, Suda H. The effect of root preparation technique and instrumentation length on the development of apical root cracks. J Endod. 2009;35(3):389-392.
- Adorno CG, Yoshioka T, Suda H. The effect of working length and root canal preparation technique on crack development in the apical root canal wall. Int Endod J. 2010;43(4):321-327.
- Ashwinkumar V, Krithikadatta J, Surendran S, Velmurugan N. Effect of reciprocating file motion on microcrack formation in root canals: an SEM study. Int Endod J. 2014;47(7):622-627.
- Barreto MS, Moraes Rdo A, Rosa RA, Moreira CH, Só MV, Bier CA. Vertical root fractures and dentin defects: effects of root canal preparation, filling, and mechanical cycling. J Endod. 2012;38(8):1135-1139.
- Bier CA, Shemesh H, Tanomaru-Filho M, Wesselink PR, Wu MK. The ability of different nickel-titanium rotary instruments to induce dentinal damage during canal preparation. J Endod. 2009;35(2):236-238.
- Bürklein S, Tsotsis P, Schäfer E. Incidence of dentinal defects after root canal preparation: reciprocating versus rotary instrumentation. J Endod. 2013;39(4):501-504.
- Capar ID, Arslan H, Akcay M, Uysal B. Effects of ProTaper Universal, ProTaper Next, and HyFlex instruments on crack formation in dentin. J Endod. 2014;40(9):1482-1484.
- Çapar ID, Uysal B, Ok E, Arslan H. Effect of the size of the apical enlargement with rotary instruments, single-cone filling, post space preparation with drills, fiber post removal, and root canal filling removal on apical crack initiation and propagation. J Endod. 2015;41(2):253-256.
- Haueisen H, Gärtner K, Kaiser L, Trohorsch D, Heidemann D (2013) Vertical root fracture: prevalence, etiology, and diagnosis. Quintessence Int. 2013;44(7):467-474.
- Al-Zaka IM. The effects of canal preparation by different NiTi rotary instruments and reciprocating WaveOne file on the incidence of dentinal defects. M Dent J. 2012;9(2):137-142.
- Kansal R, Rajput A, Talwar S, Roongta R, Verma M. Assessment of dentinal damage during canal preparation using reciprocating and rotary files. J Endod. 2014;40(9):1443-1446.
- Karataş E, Gündüz HA, Kırıcı DÖ, Arslan H, Topçu MÇ, Yeter KY. Dentinal crack formation during root canal preparations by the Twisted File Adaptive, ProTaper Next, ProTaper Universal, and WaveOne instruments. J Endod. 2015;41(2):261-264.
- Kim HC, Lee MH, Yum J, Versluis A, Lee CJ, Kim BM. Potential relationship between design of nickel-titanium rotary instruments and vertical root fracture. J Endod. 2010;36(7):1195-1199.
- Krishna VN, Suneelkumar C, Madhusudhana K, Mathew VB, Reddy A, Babu L. Evaluation of dentinal damage after root canal preparation with ProTaper Universal, Twisted Files and Mtwo rotary systems – an in vitro study. Int J Med Appl Sci. 2014;3(4):146-151.
- Kumaran P, Sivapriya E, Indhramohan J, Gopikrishna V, Savadamoorthi KS, Pradeepkumar AR. Dentinal defects before and after rotary root canal instrumentation with three different obturation techniques and two obturating materials. J Conserv Dent. 2013;16(6):522-526.
- Liu R, Kaiwar A, Shemesh H, Wesselink PR, Hou B, Wu MK. Incidence of apical root cracks and apical dentinal detachments after canal preparation with hand and rotary files at different instrumentation lengths. J Endod. 2013;39(1):129-132.
- Mahran AH, AboEl-Fotouh MM. Comparison of effects of ProTaper, HeroShaper, and Gates Glidden Burs on cervical dentin thickness and root canal volume by using multislice computed tomography. J Endod. 2008;34(10):1219-1222.
- Pop I, Manoharan A, Zanini F, Tromba G, Patel S, Foschi F. Synchrotron light-based µCT to analyse the presence of dentinal microcracks post-rotary and reciprocating NiTi instrumentation. Clin Oral Investig. 2015;19(1):11-16.
- Shemesh H, Bier CA, Wu MK, Tanomaru-Filho M, Wesselink PR. The effects of canal preparation and filling on the incidence of dentinal defects. Int Endod J. 2009;42(3):208-213.
- Topçuoğlu HS, Düzgün S, Kesim B, Tuncay O. Incidence of apical crack initiation and propagation during the removal of root canal filling material with ProTaper and Mtwo rotary nickel-titanium retreatment instruments and hand files. J Endod. 2014;40(7):1009-1012.
- Yoldas O, Yilmaz S, Atakan G, Kuden C, Kasan Z. Dentinal microcrack formation during root canal preparations by different NiTi rotary instruments and the self-adjusting file. Journal of Endodontics. 2012;38(2):232-235.
- Zandbiglari T, Davids H, Schäfer E. Influence of instrument taper on the resistance to fracture of endodontically treated roots. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006;101(1):126-131.
- Zelic K, Milovanovic P, Rakocevic Z, Askrabic S, Potocnik J, Popovic M, Djuric M. Nano-structural and compositional basis of devitalized tooth fragility. Dent Mater. 2014;30(5):476-486.
Stay Relevant With Endodontic Practice US
Join our email list for CE courses and webinars, articles and more..
