Drs. Melissa Esther Rivera-Peña, Murilo Priori Alcalde, Clóvis Monteiro Bramante, Marco Antonio Hungaro Duarte, and Rodrigo Ricci Vivan discuss periradicular surgery with simultaneous root canal filling and apical plasty
Abstract
Introduction
Periradicular surgery is an appropriate treament option for teeth with persistent periapical lesions. Among a variety of surgical techniques, simultaneous root canal filling and apical plasty are alternatives for cases with persistent exudation and periapical lesions that cannot be resolved through conventional therapy. Photodynamic therapy (PDT) is an auxiliary treatment that consists of the usage of a nontoxic photosensitizer and a soft laser application.
Objective
The purpose of this publication is to present a case in which these techniques were applied.
Methods
A clinical and radiographic evaluation was conducted on a 44-year-old male patient with a history of pulp necrosis in the upper right central incisor and of an endodontic failure in the left lateral incisor. The patient was scheduled for endodontic therapy. During the endodontic treatment of the right central incisor, the presence of continous exudate was observed throughout the appointments. Then periradicular surgery was indicated with simultaneous instrumentation and root canal filling. In the left lateral incisor, a curettage and apical plasty were performed.
Results and conclusions
Periradicular surgery with simultaneous root canal filling and apical plasty have proved to be effective modalities for the treatment of persistent periapical lesions, offering satisfactory results.
Introduction
Despite the evolution of endodontics in the past few decades, sometimes it is not possible to obtain success through conventional endodontic therapy or retreatment. These cases are classified as endodontic failures.1,2 As described by Lieblich,2 causes of endodontic failures can be associated with biologic issues, such as persistent infection, or with technical factors, such as perforations or ledging of the root canal. Consequently, periradicular surgery is an appropriate treatment option for cases that could not be resolved through conventional therapy or retreatment.2,3 Therefore, endodontic surgery should be considered as the last treatment option with the purpose of certainly resolving the pathologic issues related to the affected teeth in order to maintain their function, esthetics, and the sanity of the periradicular tissues.2,3 As a result, periradicular surgery involves meticulous treatment planning and factors that should be analyzed.2-4 Among this procedure, there are a variety of approaches and modalities for different conditions, depending on the diagnosis, anatomical structures, and prognosis. Hence, the presence of persistent periapical lesions or continous exudate, perforations, or anatomical variations are some of the indications for this procedure. Nevertheless, some aspects such as local anatomical factors, periodontal support, the possibility of restoring the tooth´s function, and the patient´s medical history should be carefully considered during the treatment planning.2-4,6 The success of this procedure also depends on the quality of the root canal filling, that should be performed with techniques and materials that can promote an ideal sealing of the root canal system.3 Lastly, among the diversity of surgical techniques, the simultaneous root canal filling is an alternative for unsolved cases with persistent exudation that cannot be resolved through conventional therapy.2,7,8 Photo-dynamic therapy (PDT) is an alternative treatment, which consists of the application of a nontoxic photosensitizer and a soft laser application, resulting in a highly reactive oxygen species and oxygenated products, inducing the injury and death of pathologic microorganisms. PDT has been studied as a promising approach to eliminate endodontic microflora.8-13 In this present case, these techniques were applied.
Materials and methods
Case report
A clinical and radiographic evaluation was conducted in a 44-year-old male patient. In the clinical and radiographic examinations, a history of pulp necrosis in the upper right central incisor (Figures 1 and 2) and a periodontal pocket with a bony defect was detected in the left lateral incisor, which was already endodontically treated (Figures 3 and 4). Therefore, the patient was scheduled for endodontic therapy in the right central incisor. After rubber dam isolation, the provisional restorative material was removed with a diamond bur, and the canal was accessed by manual instruments (K-files, Dentsply Maillefer, Ballaigues, Switzerland). The root canal was prepared with K-files applying a crown-down technique starting with a size 80 K-file and using a size 120 K-file as the last instrument (Dentsply Maillefer, Ballaigues, Switzerland); 3 mL of 1% of sodium hypochlorite was used between each instrument. Subsequently, the root canal was irrigated with sterile saline, but the presence of continuous exudate was observed. Consequently, the root canal was medicated with formocresol moistened in a sterile cotton pellet. Temporary restorations were filled with glass ionomer cement (Maxxion R, FGM, Joinville, SC, Brazil). This was observed during different appointments, hindering the conclusion of the treatment. Because of the persistence of the clinical signs, periradicular surgery was indicated, considering an apical plasty with simultaneous retro root filling of the right central incisor. In the same way, a curettage and apical plasty were suggested on the left lateral incisor because of the presence of an osseous defect surrounding the tooth. Lastly, the filling of both surgical cavities with calcium sulfate as an osseous graft was proposed.
Figures 1-4: 1. Clinical aspect of the right central incisor. 2. Radiographic image of the right central incisor. 3. Clinical aspect of the left lateral incisor. Note the presence of purulent exudate within the gingival sulcus (arrow). 4. Radiographic image of the left lateral incisor
Surgical procedures
An extraoral and intraoral cleansing with 0.12% chlorhexidine was done to lower surface bacterial load, and local anesthesia was performed with 4% articaine (1:100,000 epinephrine). A full-thickness intrasulcular rectangular flap was reflected, made with two vertical incisions extending from the maxillary right lateral incisor to the maxillary left canine by the means of a No.15c blade scalpel (Figure 5). During the surgical procedures, the presence of a bone defect in the buccal plate was observed, being used for making the ostectomy with the aid of chisels (Lucas-Triangular, Wedelstaedt, Ochsenbein/Millenium-Golgran, São Caetano do Sul, Brazil), under copious irrigation with sterile saline.
A curettage of the exposed area was executed, as well as the instrumentation of the root canal, made with K-files under copious irrigation with sterile saline. The root canal filling was performed with gutta-percha and AH Plus® endodontic sealer (Dentsply, Detrey, GmbH, Germany), using Tagger’s hybrid obturation technique. For this purpose, a master cone and two accessory gutta-percha points (XF, Dentsply Maillefer USA, Oklahoma) were placed into the root canal while performing an initial lateral compaction. Afterward, a gutta-percha condenser (No. 80, Dentsply Maillefer, Ballaigues, Switzerland) was coupled to a low-speed contra-angle handpiece and passively placed into the root canal. The gutta-percha condenser was inserted 5 mm short of the working length next to the gutta-percha cones, being activated for 3 seconds. The condenser was removed from the root canal with the contra-angle handpiece still operating while maintaining gentle pressure against one of the root canal walls. Finally, an apical plasty with the aid of an apical file (Bramante, Golgran, São Caetano do Sul, Brazil) was performed with the purpose of removing areas of roughness and smoothing the surface of the root apex.
Simultaneously, a periradicular curettage was executed on the left lateral incisor in order to remove the pathologic tissues surrounding the tooth (Figure 8). Lastly, an apical plasty was performed.
Both surgical cavities were disinfected through photodynamic therapy (MMOptics, São Carlos SP, Brazil / λ= 660 nm, P = 40 mW for 3 min, E = 7.2J) using methylene blue (Chimiolux DMC, São Carlos SP, Brazil) as a photosensitizer10 (Figure 6). Subsequently, the surgical cavities were filled with calcium sulfate (Figure 9), and the suture was done. Clinical and radiographic controls were made. Twelve months after the surgery, new bone formation could be observed radiographically, and the patient was asymtomatic (Figures 7 and 10). In the same way, cone beam computed tomography (CBCT, i-CAT™, Hatfield, Pennsylvania) images were acquired, confirming the healing of the periapical tissues, 2 years and 8 months after the surgery (Figures 11 and 12).
Results and discussion
As described by Velvart,14 the main objective of surgical treatment is to provide conditions for the healing and repair of the periradicular tissues, which is also the focus of conventional endodontic therapy.
Periradicular surgery involves a strict treatment planning and factors that should be analyzed carefully. According to different authors,2-5,7 an extensive clinical and radiographic analysis of the patients should be performed, including blood tests in order to study the case and proceed to treatment planning. Hence, anatomical structures, the presence of a periradicular lesion, and the teeth involved should be considered. Before surgery, all the potential risks should be explained to the patient in order to have his/her informed consent for all the needed procedures.2,4 Therefore, it is essential to treat the patient and not just the teeth.4
As reported by some authors,3,5,7 the selection of the flap design has an important influence under different aspects during the steps of the surgery, such as the visibility, anatomical structures, repositioning, suturing, and postoperative care. The incision chosen for this case was a full-thickness intrasulcular rectangular flap because it promotes an excellent access to the operative area. Hence, this flap design has been recommended because of its clinical advantages.2,3,7,14 Certainly, because of the variety of clinical conditions, the selection of flap design should always be made based on every individual case.14,15 It is essential to preserve epithelial and connective tissue attachment at its original level and minimize trauma during the surgical procedures in order to maintain the attachment level.16,17 For this reason, it is crucial to maintain the integrity of the papilla during restorative and surgical procedures because of the difficulty to predictably correct its height.14,17 The papilla base incision (PBI) consists of a shallow incision at the base of the papilla and a second incision directed to the crestal bone, creating a split thickness flap in the area of the papilla base.16,17 This technique has been suggested to prevent loss of interdental papilla height.16,17 However, it could be infeasible in cases where an attachment loss condition such as gingival recession is already present, as observed in this case. Some authors, have described simultaneous filling of the root canal as a useful technique in cases with an uncertain prognosis related to the presence of persistent exudate3,7,18 as well as in cases with the presence of apical resorption. This alternative has also been indicated in cases of teeth with open apex, extrusion of filling materials, anatomical variations, presence of intraradicular retainers, perforations, persistent periapical lesions, or fractured instruments within the root canal.3,19-20

Figures 5-10: 5. Full-thickness flap divulsion. 6. Disinfection of the surgical cavity with PDT. 7. Radiographic follow-up of the right central incisor (12-month control). 8. Clinical aspect of the left lateral incisor after curettage. The presence of a bony defect surrounding the tooth and apical root resorption were observed (arrow). 9. Filling of the surgical cavity with calcium sulfate. 10. Radiographic follow-up of the left lateral incisor (12-month control
According to some authors,2,4,14 peri-radicular surgery success rates have significantly evolved over the past few decades, with the improvement of retrofilling materials, ultrasonic preparation, and the use of magnification during the endodontic procedures. Periradicular surgery also offers the opportunity to retrieve tissue for histologic and microbiologic analysis,2 contributing to the diagnosis. Nevertheless, Lieblich2 explains that in cases with an expected poor success rate, such as the presence of severe periodontal bone loss with furcation involvement, the decision to extract the tooth and place an implant may be a more efficient and predictable procedure.
PDT has been studied as a promising approach to eliminate endodontic microflora.8-9, 21 In a clinical study, Juric, et al.,22 randomly selected 21 patients with endodontically treated teeth with chronic apical periodontitis in order to analyze the antimicrobial efficacy of PDT as an adjunct to conventional endodontic retreatment. Their results showed that the combination of conventional endodontic retreatment and PDT was more successful in the eradication of both gram-positive and gram-negative bacteria species as well as facultative anaerobes and obligate anaerobes when compared to retreatment alone. Therefore, photodynamic therapy could be used as an adjunct to conventional endodontic treatment. In addition, photo- dynamic therapy has been used during surgical endodontic treatment, showing promising results. Garcez, et al.,10 applied an aqueous solution of methylene blue and a diode red laser (λ= 660 nm, P = 40 mW for 3 min, E = 7.2J) in 22 patients undergoing periradicular surgery. The authors concluded that PDT associated with periradicular surgery showed superior results of microbial reduction when compared with other studies in which PDT was associated with conventional endodontic treatment.
Repair after periradicular surgery results in the formation of new tissue, involving cells and structures with the ability to react differently from the original ones. Regeneration consists of the replacement of the previous existing tissue by a new tissue identical to the former in cell composition, structure, and reactivity, implying the formation of new attachment structures.23 Because of the limitations regarding autogenous bone grafting, bone substitutes could be used to enhance osseous healing.24 The placement of calcium sulfate as a filling material in periradicular surgery has been studied by some authors,23,24 showing different results. Murashima, et al.,25 evaluated histologically and morphometrically under light and fluorescence microscope, the effect of calcium sulfate on various osseous defects in beagle dogs’ teeth undergoing apicectomy. The authors concluded that the use of calcium sulfate was effective in bone regeneration on both large osseous defects and “through-and-through” osseous defects. On the other hand, it was less efficient in defects communicating with the gingival sulcus, confirming the presence of new bone completely filling the osseous defects after 16 weeks. In addition, Pecora, et al.,23 demonstrated that the addition of calcium sulfate as a bone graft during conventional surgical treatment of through-and-through lesions improves the clinical outcome. According to the authors, further histological analysis should be done to investigate the quality of the tissues observed after the surgical procedures. In contrast to these findings, Apaydin and Torabinejad,25 found that the placement of calcium sulfate in osteotomy sites after periradicular surgery did not significantly affect alveolar healing.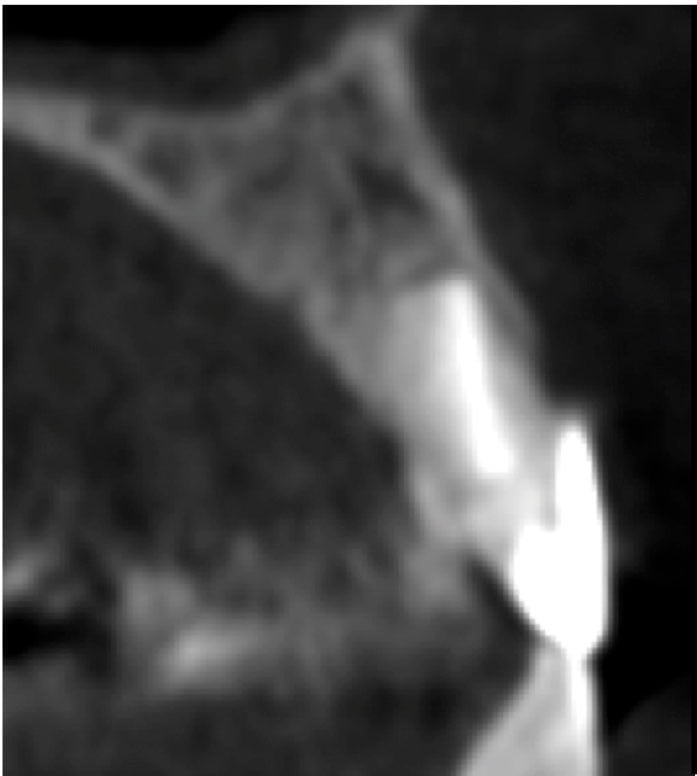 Figure: 11. Tomographic follow-up of the rigth central incisor (2-year and 8-month control).
Figure: 11. Tomographic follow-up of the rigth central incisor (2-year and 8-month control).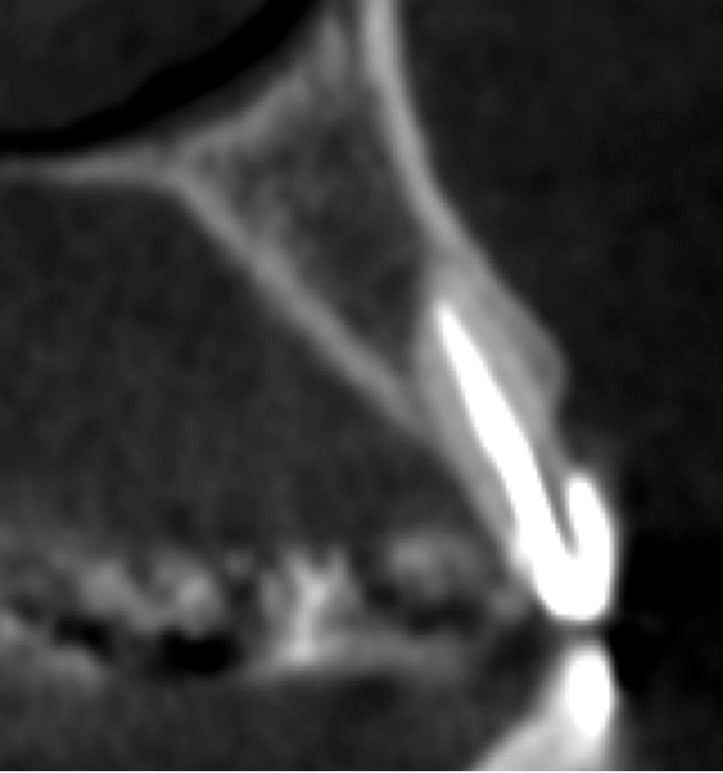 Figure: 12. Tomographic follow-up of the left lateral incisor (2-year and 8-month control)
Figure: 12. Tomographic follow-up of the left lateral incisor (2-year and 8-month control)
Ultimately, the patient’s follow-up is crucial for evaluating the development of the case and to assess the healing of the soft and periradicular tissues. This would depend on the surgeon’s ability to manipulate the tissues during the operative stages, on the patients care after the surgery, and on the patients’ immune systems response. As described by Lieblich,2 a proper follow-up protocol should be based on a radiographic and clinical evaluation 3 months after the surgery, comparing these findings with the immediate postoperative radiographic films. Documenting the case before and after with photographs should be an interesting approach as well, in order to compare the healing of the soft tissues. However, if significant bone formation has not been observed, another evaluation should be performed 6 months after the surgery. For this reason, it is of great importance to carefully choose the cases for this procedure as well as to select the best treatment modality for each case independently.4
Conclusions
Periradicular surgery with simultaneous root canal filling and apical plasty have proved to be effective modalities for the treatment of cases in which it is not possible to execute the root canal filling during the conventional endodontic treatment (continous exudate, persistent periapical lesions), offering satisfactory results. Every case should be approached based on the clinical, radiographic and tomographic findings, considering the patient’s overall health, and applying techniques supported by scientific sources.
 Melissa Esther Rivera-Peña, DDS, graduated from the Pontificia Universidad Católica Madre y Maestra (PUCMM) in Santiago de los Caballeros, Dominican Republic. She attended the Bauru School of Dentistry (FOB), University of São Paulo (USP) (Bauru, Brazil) for her specialty formation in Endodontics. At the moment, Dr. Rivera-Peña is a master’s student of the Department of Operative Dentistry, Endodontics and Dental Materials at the Bauru School of Dentistry (FOB/USP).
Melissa Esther Rivera-Peña, DDS, graduated from the Pontificia Universidad Católica Madre y Maestra (PUCMM) in Santiago de los Caballeros, Dominican Republic. She attended the Bauru School of Dentistry (FOB), University of São Paulo (USP) (Bauru, Brazil) for her specialty formation in Endodontics. At the moment, Dr. Rivera-Peña is a master’s student of the Department of Operative Dentistry, Endodontics and Dental Materials at the Bauru School of Dentistry (FOB/USP).
Murilo Priori Alcalde, MSc, is a PhD candidate of the Department of Operative Dentistry, Endodontics and Dental Materials at the Bauru School of Dentistry.
Clóvis Monteiro Bramante, PhD, is a Senior Professor of the Department of Operative Dentistry, Endodontics and Dental Materials at Bauru School of Dentistry.
Marco Antonio Hungaro Duarte, PhD, is Head Professor of the Department of Operative Dentistry, Endodontics and Dental Materials at Bauru School of Dentistry.
Rodrigo Ricci Vivan, PhD, is Professor of the Department of Operative Dentistry, Endodontics and Dental Materials at Bauru School of Dentistry.
Disclosure: Authors deny any conflict of interest or financial disclosure.
- Bernabé PFE, Holland R. Cirurgia paraendodôntica: quando indicar e como realizá-la. In: Gonçalves EA, Feller C, eds. Atualização na clínica odontológica. São Paulo, Brazil: Artes Médicas;1998:217-254.
- Lieblich SE. Current concepts of periapical surgery. Oral Maxillofacial Surg Clin North Am. 2015;27(3):383-392.
- Bramante CM, Berbert A. Cirurgia paraendodôntica. São Paulo, Brazil: Editora Santos; 2000.
- Lopes HP, Siqueira Jr JF. Endodontia: Biologia e técnica. 4th ed. Rio de Janeiro, Brazil: Elsevier; 2015.
- Tsurumachi T. Current strategy for successful periradicular surgery. J Oral Sci. 2013;55(4):267-273.
- Serrano-Giménez M, Sánchez-Torres A, Gay-Escoda C. Prognostic factors on periapical surgery: a systematic review. Med Oral Patol Oral Cir Bucal. 2015;20(6):e715-e722.
- Orosco FA, Pereira LCG, Endo MM, Rangel RA, Bramante AS, Bramante CM. Endodontic surgery with simultaneous root canal filling: case report. RSBO. 2014;11(4):411-416.
- Bonsor SJ, Nichol R, Reid TM, Pearson GJ. Microbiological evaluation of photo-activated disinfection in endodontics (an in vivo study). Br Dent J. 2006;200(6):337-341.
- Bonsor SJ, Pearson GJ. Current clinical applications of photo-activated disinfection in restorative dentistry. Dent Update. 2006;33(3):143-144, 147-150, 153.
- Garcez AS, Arantes-Neto JG, Sellera DP, Fregnani ER. Effects of antimicrobial therapy and surgical endodontic treatment on the bacterial load reduction and periapical lesion healing. Three years follow up. Photodiagnosis Photodyn Ther. 2015;12(4):575-580.
- Prażmo EJ, Kwaśny M, Łapiński M, Mielczarek A. Photodynamic therapy as a promising method used in the treatment of oral diseases. Adv Clin Exp Med. 2016;25(4):799-807.
- Silva LA, Novaes AB Jr, de Oliveira RR, Nelson-Filho P, Santamaria M Jr, Silva RAB. Antimicrobial photodynamic therapy for the treatment of teeth with apical periodontitis: a histopathological evaluation. J Endod. 2012;38(3):360–366.
- Xhevdet A, Stubljar D , Kriznar I, et al. The disinfecting efficacy of root canals with laser photodynamic therapy. J Lasers Med Sci. 2014;5(1):19-26.
- Velvart P. Papilla base incision: a new approach to recession-free healing of the interdental papilla after endodontic surgery. Int Endod J. 2005;31(1):4-16.
- Borle RM. Textbook of Oral and Maxillofacial Surgery. New Delhi, India: Jaypee Brothers Medical Publishers; 2014.
- Velvart P. Papilla base incision: a new approach to recession-free healing of the interdental papilla after endodontic surgery. Int Endod J. 2002; 35(5):453-460.
- Velvart P, Ebner-Zimmermann U, Ebner JP. Comparison of papilla healing following sulcular full-thickness flap and papilla base flap in endodontic surgery. Int Endod J. 2003;36(10):653-659.
- Kuga MC, Okamoto T, Brito JRO, Ribeiro Júnior PD, Tanaka H. Cirurgia paraendodôntica com obturação simultânea dos canais radiculares. Rev Assoc Paul Cir Dent. 1992;46(4):817-820.
- Allgayer S, Bertoglio CRS. Remoção de núcleo intrarradicular seguida de obturação do canal radicular simultânea à cirurgia apical: oito anos de proservação. RFO. 2011;16(2):211-216.
- Pinto MSC, Ferraz MAAL, Falcão CAM, Matos FTC, Pinto ASB. Cirurgia paraendodôntica: revisão da literatura. NOVAFAPI. 2011;4(4):55-60.
- Yildirim C, Karaarslan ES, Ozsevik S, Zer Y, Sari T, Usumez A. Antimicrobial efficiency of photodynamic therapy with different irradiation durations. Eur J Dent. 2013; 7(4):469-473.
- 22. Jurič IB, Plečko V, Pandurić DG, Anić I. The antimicrobial effectiveness of photodynamic therapy used as an addition to the conventional endodontic re-treatment: a clinical study. Photodiagnosis Photodyn Ther. 2014;11(4):549-555.
- Pecora G, De Leonardis D, Ibrahim N, Bovi M, Cornelini R. The use of calcium sulphate in the surgical treatment of a ´through and through´ periradicular lesion. Int Endod J. 2001;34(3):189-197.
- Apaydin ES, Torabinejad M. The effect of calcium sulfate on hard-tissue healing after periradicular surgery. J Endod. 2004;30(1):17-20.
- Murashima Y, Yoshikawa G, Wadachi R, Sawada N, Suda H. Calcium sulphate as a bone substitute for various osseous defects in conjunction with apicectomy. Int Endod J. 2002;35(9):768-774.
Stay Relevant With Endodontic Practice US
Join our email list for CE courses and webinars, articles and more..
