Dr. Robert Slosberg’s patient returns to the office for her 18-month follow-up appointment

Abstract
A patient presented with advanced internal root resorption of tooth No. 9. The prominent location of this tooth meant the case would be a challenge from an esthetic standpoint; an implant-supported crown would have been cost-prohibitive, and veneers would have been necessary to give the patient satisfactory cosmetic results. This option required too much of a cost and time commitment from the patient.
[userloggedin]
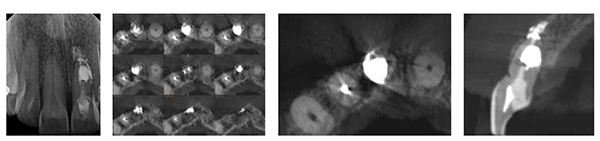
The initial treatment plan included filling the tooth with an orthodontic-grade root filling material to be followed by surgery. Visualization from a cone beam computed tomography (CBCT) scan provided accurate mapping of the defect, revealing the apical lingual perforation. Postoperatively, the CBCT scan confirmed the successful permeation of the filling material.
This case could not have been treated successfully without the use of the CBCT, both pre- and postoperatively. Placing the medication to obturate the tooth was difficult, yet the CBCT scans provided guidance allowing for measurement of the progress throughout the case. Dental radiographs offer only a 2D representation of the 3D spatial relationship, while CBCT scans allow the clinician to see every angle of a case before they even begin to operate.
Introduction
A healthy, asymptomatic 50-year-old female presented at my office in the spring of 2014, having been referred by her general practitioner. A resorption defect had been discovered during a routine periapical examination of tooth No. 9.
Because of the prominent location, it was clear from an esthetic standpoint that it would be a challenge to replace the tooth. In fact, treatment options were heavily influenced by both esthetics and the finances of the patient. An implant-supported crown and veneers may not have given the patient a satisfactory esthetic result. Additionally, such extensive work would have required a greater financial commitment from the patient.
The initial treatment plan was to fill the tooth with a conventional orthodontic-grade root filling material to be most likely followed by surgical debridement; at the time, it seemed that surgery was indeed the only option. However, as we would discover, CBCT technology provided accurate mapping and obturation of the defect, eliminating the need for surgery, at least for now.





Clinical and radiographic examination
The resorptive defect — the patho-logical process in which the tooth begins to dissolve — was initially diagnosed by radiograph; however, the CBCT scan showed the exact extent of the defect, as well as revealed an apical lingual perforation, which presented yet another challenge.
- Medical history: Non-contributory
- Diagnosis: Advanced internal root resorption
- Immediate treatment plan: Canal obturation and filling
Treatment
A coronal access opening was made, and the tooth was packed with calcium hydroxide. This proved challenging as controlling placement of the calcium hydroxide was particularly difficult. A temporary filling was then placed, and the medication was changed over the course of 2 to 3 months. CBCT scans were taken postoperatively to determine where the medication was and where it wasn’t. On the advice of a colleague, the access opening was extended toward the lingual to facilitate the vertical condensation of the root filling material — in this case, Brasseler bioceramic mineral trioxide aggregate (MTA) cement. On top of the EndoSequence® BC RRM™ (Root Repair Material) and EndoSequence® BC Sealer™, a composite resin core buildup of exactly 10 mm deep was placed.


Results
CBCT scans allowed for accurate mapping of the defect, and they were the only way to assess the effective permeation of the bioceramic putty.
Discussion
Due to the many challenges this case presented, the mapping of the defect was shared among endodontic professionals — trusted colleagues, local study clubs, and endodontic online forums. The majority of the dental professionals recommended extraction and an implant-supported crown.
Esthetics and finances directed this individualized treatment plan. Filling the tooth — even if it were maintained for up to 5 years — would allow the patient time to save enough money for an implant-supported crown. For ideal esthetics with an implant-supported crown, at least one or more veneers would most likely be necessary; therefore, a steep financial and time commitment would be required from the patient. Surgery was always an option, depending on the outcome of endodontic therapy.
This case could not have been treated successfully without the use of CBCT scans. In fact, the patient was referred specifically to our practice because we are known for our use of CBCT technology. CBCT gives us additional information that conventional 2D radiographs cannot. In this case, it facilitated both accurate mapping and obturation of the resportive defect. The scans can answer important questions such as “Can the defect be reached?” Once completed, CBCT answers, “How adequately was the tooth sealed?”
In this particular case, CBCT scans were crucial in confirming the placement of the calcium hydroxide and the bioceramic resin. Placing the medication was a challenge, and CBCT scans measured the progress throughout the case. A CBCT scan can also be a professional’s worst critic. The scan will reveal, “You didn’t get the calcium, medication, or filling material here.” In conclusion, it was a CBCT scan that confirmed the successful condensation of the bioceramic putty used to seal the tooth, and surgery was avoided, at least, in the short term. The patient is asymptomatic and is due for a recall.
In the modern endodontic office, CBCT is a powerful new tool to aid in the diagnosis and treatment of diseases involving the teeth and supporting structures. Dental radiographs can only offer a 2D representation of the 3D spatial relationship. However, today’s specialists can understand that spatial relationship better with the advent of CBCT.
Following a detailed clinical evaluation, including radiographs, it may be necessary to gain more information — information that only CBCT scans can provide. CBCT technology provides a complete visual image covering the axial, coronal, and sagittal planes. Additionally, the 3D rendering is also an excellent tool for patient education and can lead to increased case acceptance.
The advent of CBCT and its subsequent introduction into the endodontic specialty have been a paradigm shift. The more scans I have reviewed, the more I realize just how important a 3D scan can be to comprehensive diagnosis; at this point, CBCT scans are taken for most of my endodontic cases, as they can solve the mysteries that are left uncovered by 2D radiography.
Returning to the case at hand: “If it were your patient, what would you recommend? Even more importantly, if it were your tooth, how would you want it treated?”
Lessons learned
- Extending the access opening lingually was not ideal, though it was necessary to adequately condense the bioceramic putty.
- In hindsight, the tooth could have been strengthened had a fiber post been placed along with composite resin.
- Recent technological advancements in Endodontics have made treatment options possible, that were not available just a few years ago.
18-month recall
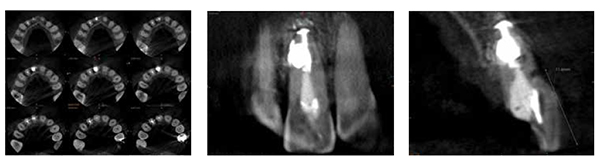
At an 18-month recall appointment, the patient has remained asymptomatic. Clinically, probing depths were WNL, and the tooth has remained esthetically pleasing. On the new cone beam, the periapical area, as well as the lateral aspect of the sealed defect, is suggestive of periapical healing. No new defects were noted internally. The patient was dismissed and placed on a 1-year recall.
A closer look at the CBCT scan, however, is suggestive of a resorptive defect on the buccal surface, approximately 11 mm from the incisal edge. What would you do next?


[/userloggedin]
[userloggedout][/userloggedout]
Stay Relevant With Endodontic Practice US
Join our email list for CE courses and webinars, articles and more..
