Drs. O.A. Hafez, A.H. Diab, and H.A. El Asfouri explore file systems and postoperative pain in different file systems.
Drs. O.A. Hafez, A.H. Diab, and H.A. El Asfouri explore file systems and postoperative pain
Summary
Objective
To compare the intensity of postoperative pain after a single visit endodontic treatment using ProTaper® Universal multiple file system (Dentsply Sirona, Charlotte, North Carolina) and the single file rotary systems — ONE ENDO (NanoEndo LLC, Chattanooga, Tennessee) and F6 SkyTaper™ (Komet Dental, Lemgo, Germany).
Methodology
Fifty-eight patients aged between 20-50 years old were diagnosed with symptomatic irreversible pulpitis of one maxillary or mandibular premolar. Teeth were randomly assigned to three groups according to the root canal shaping system: ONE ENDO (Group A), F6 SkyTaper™ (Group B), and Rotary ProTaper® Universal (PTU) as a control (Group C). The comparison mainly focused on discovering whether single-file systems are causing the same or different levels of postoperative pain as traditionally used multiple-file systems. The PTU system was the most commonly used system with previous study reports of its performance and, therefore, was selected as a control group for the present study. All treatments were completed in a single visit. The severity of the postoperative pain was assessed by the verbal rating scale (VRS) after 24, 48, and 72 hours. Data was analyzed using the Kruskal-Wallis and Mann-Whitney U tests.
Results
After 24 hours: There was no statistically significant difference between the three studied groups (p = 0.126). After 48 hours: Group A showed the lowest pain levels with statistically significant difference with both groups B (p = 0.003) and C (p = 0.036). However, there was no statistically significant difference between the intervention group B and the control group C (p = 0.407). After 72 hours: Group A showed the highest levels of total pain relief with statistically significant difference with group B (p = 0.011) but without significant difference with group C (p = 0.073). Pain scores for both groups B and C were almost similar (p = 0.459).
Conclusion
The number of instruments had no impact on postoperative pain. The theory supporting why a clinician would expect different pain levels posttreatment based on a file system is that the number of files as well as file design can extrude different amounts of debris beyond the apex with/without significant effect on postoperative pain.
Introduction
Chemo-mechanical preparation of the root canal system is one of the prerequisites of endodontic treatment. The procedure involves canal shaping and using intracanal irrigants to provide optimal cleaning and disinfection within the root canal system. Although various methodologies have been introduced, one of the problems related to all root canal shaping and cleaning procedures is the extrusion of intracanal debris and irrigants into the peri-radicular tissues.1
Debris extrusion during root canal instrumentation is an undesirable side effect of treatment.2 Clinical and biological relevance of apical extrusion of debris is the interappointment or postoperative pain and flare-ups.1 Many studies mentioned that endodontic patients reported various degrees of pain after endodontic treatment.3 The prevalence of post-endodontic pain was estimated to be 3:58%. With the introduction of single-file systems, a single instrument is used for the entire procedure, which means that the same total amount of debris has to be contained within a single set of flutes.2 Therefore, the efficiency of single-file systems may be accompanied by drawbacks, at least regarding apical extrusion of debris and especially in infected cases where these systems may cause more interappointment emergencies.4 Recent studies have shown that the treatment protocols of new reciprocating systems can also produce extrusion of debris in the apical region, which could be related to postoperative pain when compared with other traditional instrumentation techniques.5 The highest incidence occurs during the first 24-48 hours and gradually decreases over the following days.6 It is one of the major tasks of the endodontist to avoid or minimize, as much as possible, the irritation of the periapical tissues during root canal treatment.6
Apical extrusion of debris has been associated with all types of instruments and instrumentation techniques, even when preparation is maintained short of the apical terminus with some instrumentation techniques extruding less material than others.7 Debris extruded beyond the apical foramen may result in periapical inflammation and postoperative pain. To date, no root canal preparation method has been developed that extrudes no periapical debris. The number of instruments and the kinematics of movement may contribute to debris extrusion during root canal preparation.2
ProTaper® Universal system is a well-known, engine-driven multiple-file system with continuous rotational movement. It has been the topic of many investigations concerned with apical extrusion of debris as well as its association with postoperative pain. Although it was proved in some studies8-15 to extrude debris more than many other systems, associated postoperative pain was associated with controversy.4,16-20
The newer single-file NiTi systems such as ONE ENDO21 and F6 SkyTaper22 are designed to completely prepare root canals with only one instrument. Both systems are used in a continuous rotation motion. The ONE ENDO is a new type of file design: delta-type; featuring two unequal tapers side by side within the same instrument (Figure 1). The F6 SkyTaper system is a 0.06 taper, which is a newer modification of the 0.04 taper rotary system — F36022 (Figure 2).
Presently, no previous study has evaluated the effect of the newer single-file rotary systems, ONE ENDO and F6 SkyTaper, on postoperative pain. The null hypothesis for this study stated that there is no difference in postoperative pain between the three groups.


Participants and methods
Study design and sampling
This study was a single-blinded, controlled, parallel-grouped, randomized clinical trial. All the procedures were done according to the Declaration of Helsinki (version 2008) and approved by the Research Ethics Committee, Faculty Dentistry, Cairo University, Egypt, with the approval number 16821. The trial was registered on www.ClinicalTrials.gov with the identifier: NCT03065777. All the participants signed an informed consent after understanding the treatment procedure and accepting the possible risks.
Eligibility criteria
Outpatients in the clinic of Endodontics at the Faculty of Dentistry, Cairo University, Egypt, were recruited to participate in the study according to the following eligibility criteria:
A. Inclusion criteria
All adults (20-50 years old), medically-free patients (males or females) having maxillary or mandibular premolar teeth with symptomatic irreversible pulpitis and indicated for conventional endodontic treatment who accept to enroll in the study.
B. Exclusion criteria
Those cases that fulfilled any of the following criteria were excluded: nonvital teeth; teeth with apical periodontitis; teeth requiring endodontic retreatment; root resorption; immature/open apex; root canals with radiographic evidence of calcification in which patency of the apical foramen could not be established; presence of more than one symptomatic tooth in the same quadrant; pregnancy, medically compromised patients, or patients receiving medication for chronic pain; patients who have taken analgesics in the last 12 hours before treatment; teeth that have initial apical size more than 20; and teeth that could not be treated in a single session. If any evidence of extrusion of root filling material was noticed radiographically, the case was excluded.
To confirm symptomatic irreversible pulpitis, the patients should have experienced moderate to severe pain as well as prolonged response to cold testing by Endo-Ice® (Coltene/Whaledent, Inc., Mahwah, New Jersey). Bleeding on access cavity preparation should be present. There should be no periapical radiolucency except for widening periodontal ligaments present radiographically.
Randomization
In order to randomly assign the patients, a random sequence generated by www.random.org for patients’ numbers was used to assign the patients in the three groups: A, B, or C.
Clinical procedures
Root canal treatment was completed in a single visit by an endodontic master’s degree student. All patients received local anesthetic administration with 1.8 ml Mepivacaine HCl 2%-Levonordefrin 1:20000 (Alexandria company for pharmaceuticals and Chemical industries, Egypt). Levonordefrin was used as a vasoconstrictor similar to epinephrine but more stable. The affected tooth was isolated with a rubber dam; then access cavity preparation was done with round carbide and Endo-Z™ burs (Dentsply Maillefer, Tulsa, Oklahoma), using an air turbine handpiece and underwater coolant. Working length was determined with a Root ZX® apex locator (J. Morita, Tokyo, Japan) (J. Morita USA Inc., Irvine, California) and confirmed radiographically. A size 10 K-File (Mani, Utsunomiya, Japan) was used as a patency file. Initial apical size was confirmed to be 20 before introducing the rotary files.
For the ONE ENDO group, coronal flaring was done using an OP10L19 orifice opener (Komet Dental, Lemgo, Germany) at speed 300 rpm and 2.8 Ncm. Then a size 30/0.06 ONE ENDO file (NanoEndo LLC, Chattanooga, Tennessee) at 500 rpm was used at WL with a gentle picking motion. For the F6 SkyTaper group, coronal flaring was done using a OP10L19 orifice opener. Then a size 30/0.06 F6 SkyTaper file (Komet Dental, Lemgo, Germany) at 300 rpm and 2.2 Ncm torque was used at WL with gentle picking motion. For the ProTaper Universal (PTU) group, the following sequence was used: SX, S1, S2, F1, F2, and F3 files according to the manufacturer’s instructions for speed and torque of each file. All the three rotary systems were mounted on 16:1 reduction handpiece operated by the X-Smart® Endo Motor (Dentsply Maillefer, Ballaigues, Switzerland) (Dentsply Maillefer, Tulsa, Oklahoma), and introduced into the canal with EDTA gel (MD-Chelcream, META BIOMED CO., LTD, Korea) as a lubricant.
The root canals were abundantly irrigated with 2 ml of 5.25% sodium hypochlorite (NaOCl) after each instrument exchange using the 30-guage needle up to 1 mm short of the working length. The amount of final irrigating solution was 10 ml NaOCl and 2 ml EDTA 17% (Master-Dent® EDTA solution; Dentonics, Charlotte, North Carolina) for each canal. Prior to obturation, the root canals were completely dried using 95% ethyl alcohol and sterile absorbent paper points compatible with the root canal diameters. According to Stevens, et al.,23 drying of the canals using 95% ethyl alcohol leads to better uniform adherence of the sealer to dentin surface and penetration of sealer into dentinal tubules. The gutta-percha master cone, compatible with the root canal instrumentation, was then inserted into the root canal, and the first 5 mm was coated with ADSEAL resin sealer (META BIOMED CO., LTD, Korea). Obturation of the root canal system was performed by the single cone or modified single cone techniques. Upon completion of the obturation, the tooth was filled with temporary filling material (Tfil; AHL, Ltd, Kent, UK), and then occlusal adjustment was done (completely taken out of occlusion).
Patients were informed that they could experience pain in the days following treatment and asked to fill out a verbal rating scale (VRS)24 defined as follows:
- No pain.
- Mild pain: any discomfort of any duration that does not require analgesics.
- Moderate pain: pain that requires and is relieved with analgesics.
- Severe pain: any pain that is not relieved with analgesics.
To assess postoperative pain, a scale of pain intensity was applied 24 hours, 48 hours, and 72 hours after endodontic treatment after telephoning the research individuals. The recommended medication for pain was ibuprofen (400 mg) when needed.
 Statistical analysis
Statistical analysis
Data was analyzed using IBM SPSS advanced statistics (Statistical Package for Social Sciences), version 21 (SPSS Inc., Chicago, Illinois). Numerical data was described as mean and standard deviation or median and range. Data was explored for normality using the Kolmogrov-Smirnov test and Shapiro-Wilk test. Comparisons between study groups for normally distributed numeric variables were done using the ANOVA, followed by Bonferoni post hoc test. Non-normally distributed numeric variables were done by Kruskal-Wallis test, and pairwise comparisons were done by Mann Whitney test. Comparisons between categorical variables were performed using the chi-square test. A p-value less than or equal to 0.05 was considered statistically significant. All tests were two-tailed.
Results
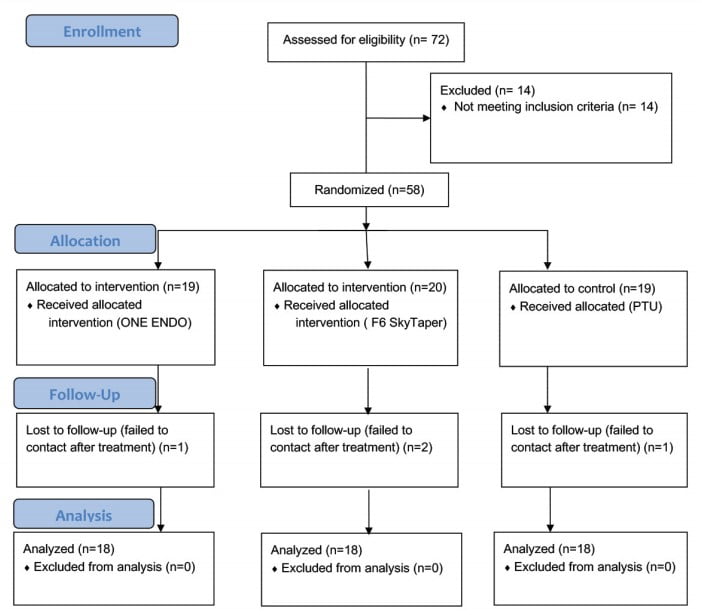
A total of 72 patients was assessed to enroll in this study. Fourteen patients were excluded due to expressing one or more of the exclusion criteria. Fifty-eight patients were enrolled to participate in one of the three groups. There was failure to contact with four patients (i.e., one patient in group A, two patients in group B, and one patient in group C). Statistical analysis was performed on the remaining 54 participants. The flow chart of the patients through the study followed the CONSORT flow diagram (Chart 1).
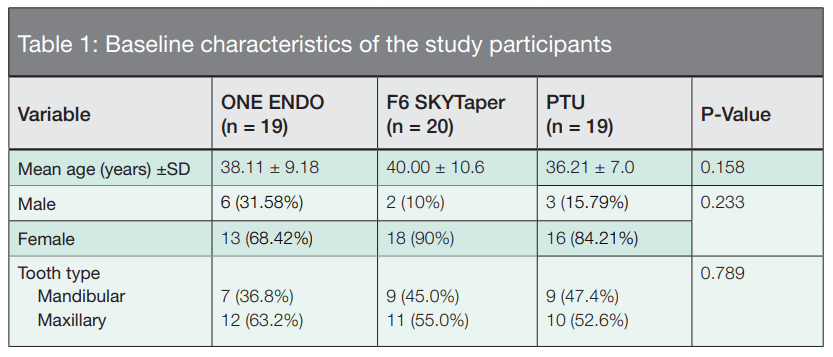
Table 1 summarizes the demographic data and general characteristics of the study groups. There were no significant differences in age, gender, type of teeth, or the number of canals between the three groups (p > 0.05).
Outcome
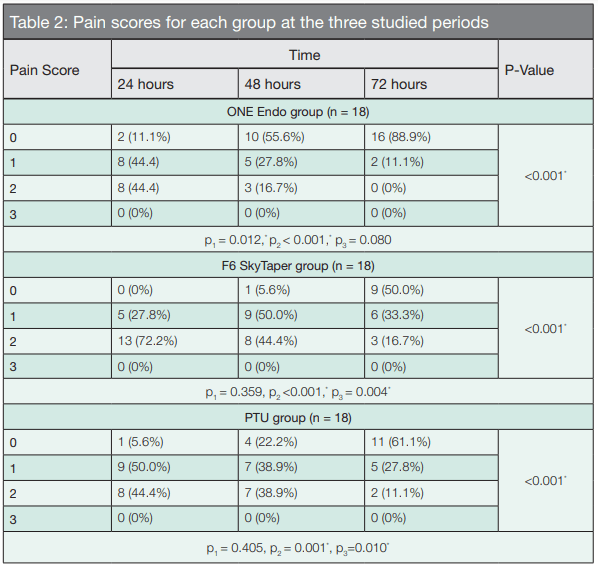
Table 2 describes pain scores for each group at the three studied periods. Group A: There was significant decrease of pain levels after 48 hours (p = 0.012). However, there was no significant difference after 72 hours (p = 0.080). Group B: There was no significant decrease in pain levels in the first 2 days (p = 0.359) but there were significant lower pain scores after 72 hours (p = 0.004). Group C: Results were similar to group B as there was no significant decrease of pain scores at the first 2 days (p = 0.405), and the lowest pain scores were significantly expressed after 72 hours (p = 0.010).
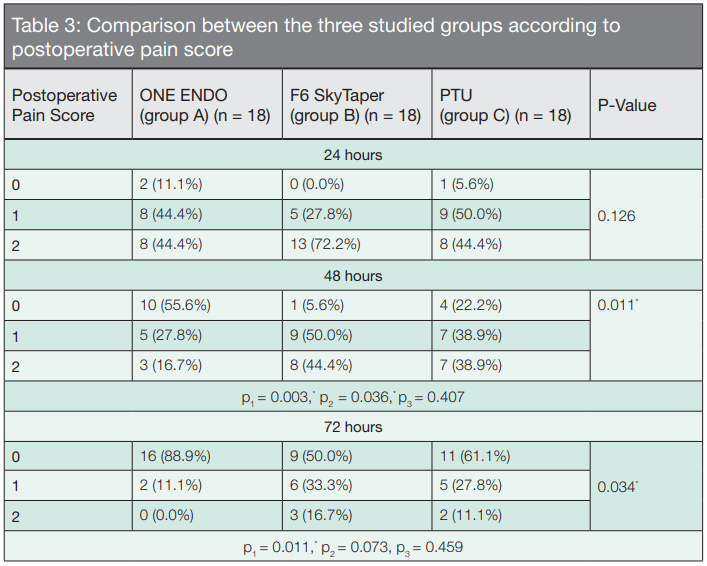
Table 3 illustrates the comparison of postoperative pain scores between the three groups at different follow-up periods. After 24 hours: There was no statistically significant difference between the three studied groups (p = 0.126). After 48 hours: Group A showed the lowest pain levels with statistically significant difference with both groups B (p = 0.003) and C (p = 0.036). However, there was no statistically significant difference between group B and group C (p = 0.407). After 72 hours: Group A showed the highest levels of total pain relief (i.e.: pain score 0) with statistically significant difference with group B (p = 0.011) but without significant difference with group C (p = 0.073). Pain scores for both groups B and C were almost similar (p = 0.459).
p2: p value for comparing between 24 hours and 72 hours
p3: p value for comparing between 48 hours and 72 hours *
Statistically significant at p ≤ 0.05
p2: p value for comparing between Group A and Group C
p3: p value for comparing between Group B and Group C
* Statistically significant at p ≤ 0.05
Discussion
The aim of this clinical trial was to compare the effect of using single file rotary systems; ONE ENDO and F6 SkyTaper with the conventional multi-file rotary ProTaper Universal system on postoperative pain in cases diagnosed with symptomatic irreversible pulpitis. The results showed that after 24 hours, the highest incidence of moderate pain was in cases treated by the F6 SkyTaper system although the difference was not significant among the assessed instrumentation systems. After 48 hours, significantly lower pain scores were noticed in the ONE ENDO group than the F6 SkyTaper and ProTaper Universal groups, while higher pain levels were associated with the F6 SkyTaper system but without significant difference when compared to the control group. After 72 hours, 16 patients treated by the ONE ENDO system reported total relief of pain with significant difference to the other two groups. Nine and 11 patients in F6 SkyTaper and ProTaper Universal groups, respectively, reported absence of pain without significant difference between them. Regarding the ONE ENDO system, the null hypothesis was rejected while we failed to reject the hypothesis for the F6 SkyTaper system.
For the present study, the highest pain scores in all the three groups occurred in the first 24 hours, with gradual reduction in pain levels at the following follow-up periods of 48 hours and 72 hours. Similar findings were reported in a systematic review by Pak, et al.,25 in which pain incidence in the first 24 hours was 40%, declining sharply thereafter, particularly over the first 2 days, and reaching levels of 11% at 7 days. Kherlakian, et al.,26 and Mollashahi, et al.,27 mentioned similar results when using one of the instrumentation systems ProTaper Next, WaveOne® (Dentsply Sirona) or RECIPROC (VDW, Munich, Germany) in the former study or RECIPROC and One Shape files (Medidenta, Las Vegas, Nevada) in the latter.
Lower pain levels reported in the ONE ENDO group may be attributed to the file’s special design. It has a cut-flip tip resembling a thick spoon with a sharpened edge. The tip’s blade effectively forms dentinal chips while its opposite side is a curved surface acting as a self-guiding pilot resulting in a flexible tip that can enlarge canals smaller than its tip size effectively with less stress and less debris extrusion.21 The two unequal tapers, side by side, incorporated in the ONE ENDO file afford it superior flexibility and an improved ability to remove debris.21 While its larger tapered cutting edge engages the canal wall, provides superior strength, and superior cutting efficiency, its opposing smaller tapered edge provides additional space for breaking down and removing debris. Furthermore, the ONE ENDO file features fewer spirals at the tip to resist screwing-in forces21 (Figure 3).
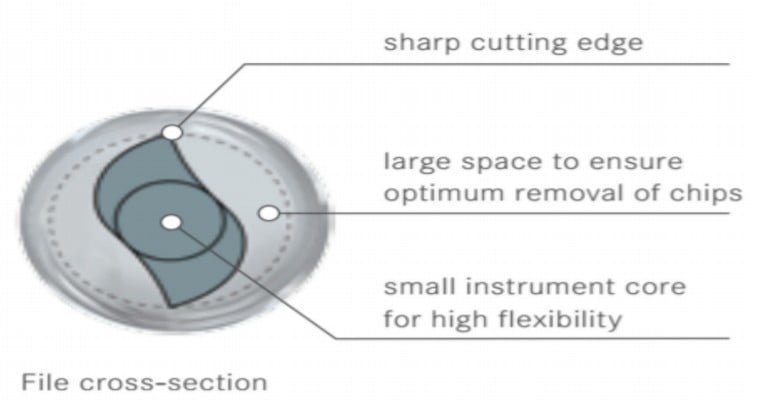
F6 SkyTaper file has S-shaped a cross-sectional design, which gives the instrument small core diameter with two sharp cutting blades and deep flutes creating a space for debris accumulation (Figure 4). However, this cross section is the same through the whole length of the file (i.e., fixed cross section); and besides its constant 0.06 taper, this design may render the system of better cutting efficiency and higher tendency to screw-in and push internal canal debris beyond the apex.22 Clinically, this was reflected in the present study through higher expression of pain 2 and 3 days postoperatively with significant difference to the ONE ENDO group. On the other hand, no significant difference was noticed at any time interval between the F6 SkyTaper system and the ProTaper Universal system.
The ProTaper Universal system, which served as control group for the present study, is a more conventionally used full-sequence rotary system. It provides a slower mechanical enlargement and gradual approach to the apex. Recent studies were more concerned with investigating the single-file reciprocating systems than continuously rotating ones. That is why the present study aimed to compare the multi-file system with the newly introduced single-file rotating ones regarding their influence on postoperative pain. The convex triangular cross section of the ProTaper Universal shaping files and finishing files F1 and F2 provides greater mass to the instruments’ core, making them more rigid, reducing the depth of flutes, and therefore limiting its ability to allow coronal removal of debris. The cross section of larger finishing files was modified to be concave triangular to make them more flexible; however, these concave areas do not provide sufficient space for debris accumulation. Using a sequence of files gradually approaching the apex may compensate for this limitation.28
By searching the recent available literature, no clinical studies were published incorporating either the ONE ENDO system or the F6 SkyTaper, although ProTaper Universal was compared to single-file reciprocating systems. Pasqualini et al.,17 and Nekoofar et al.,29 reported significant lower postoperative pain in patients treated by ProTaper Universal system than those who treated by the single file reciprocating system, WaveOne. However, Shokraneh, et al.,19 reported that postoperative pain was significantly lower in patients undergoing root canal instrumentation with the WaveOne file compared with the ProTaper Universal files. Relvas, et al.,4 concluded that the occurrence of postoperative pain was similar between Reciproc system and rotary ProTaper Universal system during the time intervals assessed.
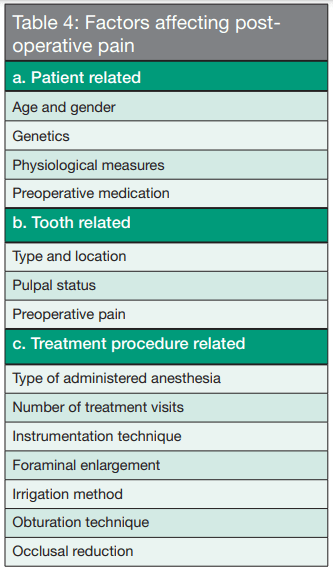
Several factors are involved in the sensation of postoperative pain (Table 4). This makes clinical investigations that associate pain incidence with possible causes more challenging.26 Although mild discomfort is generally expected after undergoing endodontic treatment, the incidence of postoperative pain and flare-up is reported to range from 3:58%.5 Mechanical, chemical, or microbial injuries to periapical tissues are the leading causes of acute periapical inflammation.30 Preoperative pain is one of the strongest predictors of postoperative pain.31 Therefore, only teeth with vital pulp diagnosed with symptomatic irreversible pulpitis and indicated for endodontic treatment were selected for the present study. In addition, all the teeth were treated in a single visit to rule out the potential influence of intracanal medication or other factors triggering pain.
After access cavity preparation, cervical preflaring was done using the orifice opener OP10L file for both intervention groups. Borges, et al.,32 reported that cervical preflaring was associated with significantly lesser amount of apically extruded debris when used with different instrumentation systems. All rotary files were introduced into the canals with EDTA gel to reduce heat generated by the rotating instrument against dentinal walls as well as removal of the smear layer.
According to the conditions established for this study, there were no statistically significant differences regarding the gender and age between the three studied groups. These results are in agreement with Watkins, et al.,33 Segura-Egea, et al.,34 and Sadaf, et al.,35 who reported that males and females reported the same level of pain. On the other hand, contrary to the results of the present study, Watkins, et al.33 and Segura-Egea, et al.,34 reported that younger people experienced significantly higher pain levels.
With regards to the tooth type whether maxillary or mandibular premolars, results of the present study go with conclusions reported by Watkins, et al.,33 Segura-Egea, et al.,34 and Harrison, et al.,36 as there was no significant difference between maxillary and mandibular premolar teeth.

Conclusion
Within the limitations of the present study, it could be concluded that the number of root canal shaping files may not have a significant effect on the postoperative pain.
File systems and postoperative pain in a single-visit RCT are the focus of this CE article. Take the free CE quiz and receive 2 credits! https://endopracticeus.com/ce-articles/occurrence-of-post-endodontic-pain-after-single-visit-rct-using-balanced-force-technique-and-two-reciprocating-systems-when-apical-patency-ap-is-maintained/
- Tanalp J, Güngör T. Apical extrusion of debris: a literature review of an inherent occurrence during root canal treatment. Int Endod J. 2014;47(3):211-221.
- Farmakis ETR, Sotiropoulos GG, Abràmovitz I, Solomonov M. Apical debris extrusion associated with oval shaped canals: a comparative study of WaveOne vs Self-Adjusting File. Clin Oral Investig. 2016;20(8):2131-2138.
- Ince B, Ercan E, Dalli M, Dulgergil CT, Zorba YO, Colak H. Incidence of postoperative pain after single- and multi-visit endodontic treatment in teeth with vital and non-vital pulp. Eur J Dent. 2009;3(4):273-279.
- Relvas JBF, Bastos MMB, Marques AAF, Garrido ADB, Sponchiado EC. Assessment of postoperative pain after reciprocating or rotary NiTi instrumentation of root canals: a randomized, controlled clinical trial. Clin Oral Investig. 2016;20(8):1987-1993.
- Sathorn C, Parashos P, Messer H. The prevalence of postoperative pain and flare-up in single- and multiple-visit endodontic treatment: a systematic review. Int Endod J. 2008;41(2):91-99.
- Caviedes-Bucheli J, Castellanos F, Vasquez N, Ulate E, Munoz HR. The influence of two reciprocating single-file and two rotary-file systems on the apical extrusion of debris and its biological relationship with symptomatic apical periodontitis. A systematic review and meta-analysis. Int Endod J. 2015;49:1-16.
- Soi S, Yadav S, Sharma S, Sharma M. In Vitro Comparison of Apically Extruded Debris during Root Canal Preparation of Mandibular Premolars with Manual and Rotary Instruments. J Dent Res Dent Clin Dent Prospects. 2015;9(3):131-137.
- Tanalp J, Kaptan F, Sert S, Kayahan B, Bayirl G. Quantitative evaluation of the amount of apically extruded debris using 3 different rotary instrumentation systems. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006;101(2):250-257.
- Taşdemir T, Er K, Çelik D, Aydemir H. An in vitro comparison of apically extruded debris using three rotary nickel-titanium instruments. J Dent Sci. 2010;5(3):121-125.
- Surakanti JR, Venkata RCP, Vemisetty HK, et al. Comparative evaluation of apically extruded debris during root canal preparation using ProTaperTM, HyflexTM and WaveoneTM rotary systems. J Conserv Dent. 2014;17(2):129-132.
- Capar ID, Arslan H, Akcay M, Ertas H. An in vitro comparison of apically extruded debris and instrumentation times with ProTaper Universal, ProTaper Next, Twisted File Adaptive, and HyFlex instruments. J Endod. 2014;40(10):1638-1641.
- Koçak MM, Çiçek E, Koçak S, Sağlam BC, Furuncuoğlu F. Comparison of ProTaper Next and HyFlex instruments on apical debris extrusion in curved canals. Int Endod J. 2016;49(10):996-1000.
- Ozsu D, Karatas E, Arslan H, Topcu MC. Quantitative evaluation of apically extruded debris during root canal instrumentation with ProTaper Universal, ProTaper Next, WaveOne, and self-adjusting file systems. Eur J Dent. 2014;8(4):504-508.
- Cakici F, Cakici EB, Küçükekenci FF, Uygun AD, Arslan H. Apically extruded debris during root canal preparation using ProTaper Gold, ProTaper Universal, ProTaper Next, and RECIPROC instruments. Int J Artif Organs. 2016;39(3):128-131.
- Karataş E, Ersoy İ, Gündüz HA, et al. Influence of instruments used in root canal preparation on amount of apically extruded debris. Artif Organs. 2016;40(8):774-777.
- Arias A, de la Macorra JC, Azabal M, Hidalgo JJ, Peters OA. Prospective case controlled clinical study of post-endodontic pain after rotary root canal preparation performed by a single operator. J Dent. 2015;43(3):389-395.
- Pasqualini D, Corbella S, Alovisi M, et al. Postoperative quality of life following single-visit root canal treatment performed by rotary or reciprocating instrumentation : a randomized clinical trial. Int Endod J. 2016; 49(11):1030-1039.
- Krithikadatta J, Sekar V, Sudharsan P, Velumurugan N. Influence of three Ni-Ti cleaning and shaping files on postinstrumentation endodontic pain: A triple-blinded, randomized, controlled trial. J Conserv Dent. 2016;19(4):311–6.
- Shokraneh A, Ajami M, Farhadi N, Hosseini M, Rohani B. Postoperative endodontic pain of three different instrumentation techniques in asymptomatic necrotic mandibular molars with periapical lesion: a prospective, randomized, double-blind clinical trial. Clin Oral Investig. 2017;21(1):413-418.
- Shahi S, Asghari V, Rahimi S, et al. Postoperative pain after endodontic treatment of asymptomatic teeth using rotary instruments: a randomized clinical trial. Iran Endod J. 2016;11(1):38-43.
- NanoEndo. https://nanoendo.com/index.php#. Accessed on February 19, 2020.
- Dagna A, Gastaldo G, Beltrami R, Chiesa M, Poggio C. F360 and F6 Skytaper: SEM evaluation of cleaning efficiency. Ann Stomatol (Roma). 2016;6(1):69-74.
- Stevens RW, Strother JM, McClanahan SB. Leakage and sealer penetration in smear-free dentin after a final rinse with 95% ethanol. J Endod. 2006;32(8):785-788.
- Coll AM, Ameen JRM, Mead D. Postoperative pain assessment tools in day surgery: Literature review. J Adv Nurs. 2004;46(2):124-133.
- Pak JG, White SN. Pain prevalence and severity before, during, and after root canal treatment: A systematic review. J Endod. 2011;37(4):429-438.
- Kherlakian D, Cunha RS, Ehrhardt IC, et al. Comparison of the incidence of postoperative pain after using 2 reciprocating systems and a continuous rotary system: a prospective randomized clinical trial. J Endod. 2016;42(2):171-176.
- Mollashahi NF, Saberi EA, Havaei SR, Sabeti M. Comparison of postoperative pain after root canal preparation with two reciprocating and rotary single-file systems: a randomized clinical trial. Iran Endod J. 2017;12(1):15-19.
- Ruddle, Clifford J., Pierre Machtou, and John D. West. The Shaping Movement: Fifth-Generation Technology. Dent Today. 2013;32(4):22-28.
- Nekoofar MH, Sheykhrezae MS, Meraji N, et al. Comparison of the effect of root canal preparation by using waveone and protaper on postoperative pain: a randomized clinical trial. J Endod. 2015;41(5):575-578.
- Siqueira JF Jr, Barnett F. Interappointment pain: mechanisms, diagnosis and treatment. Endod Topics. 2004;7(1):93-109.
- Glennon JP, Ng Y, Setchell DJ, Gulabivala K. Prevalence of and factors affecting post-obturation pain in patients undergoing root canal treatment. Int Endod J. 2004;37(1):29-37.
- Borges ÁH, Pereira TM, Porto AN, et al. The Influence of Cervical Preflaring on the Amount of Apically Extruded Debris after Root Canal Preparation Using Different Instrumentation Systems. J Endod. 2015;42(3):465-469.
- Watkins CA, Logan HL, Kirchner HL. Anticipated and experienced pain associated with endodontic therapy. J Am Dent Assoc. 2002;133(1):45-54.
- Segura-Egea JJ, Cisneros-Cabello R, Llamas-Carreras JM, Velasco-Ortega E. Pain associated with root canal treatment. Int Endod J. 2009;42(7):614-620.
- Sadaf D, Ahmad MZ. Factors associated with postoperative pain in endodontic therapy. Int J Biomed Sci. 2014;10(4):243-247.
- Harrison JW, Baumgartner JC, Svec TA. Incidence of pain associated with clinical factors during and after root canal therapy. Part 2. Postobturation pain. J Endod. 1983;9(10):434-438.
Stay Relevant With Endodontic Practice US
Join our email list for CE courses and webinars, articles and more..
