CE Expiration Date:
CEU (Continuing Education Unit): Credit(s)
AGD Code:
Educational aims and objectives
This clinical article aims to present the clinical applications of WaveOne® Gold reciprocating instruments.
Expected outcomes
Endodontic Practice US subscribers can answer the CE questions by taking this quiz to earn 2 hours of CE from reading this article.
Correctly answering the questions will demonstrate the reader can:
- Identify the design features of WaveOne Gold reciprocating instruments, particularly the primary file, for use in root canal preparation.
- Realize the benefits of reciprocating motion.
- Realize some characteristics of M-Wire technology.
- See clinical guidelines for the use of WaveOne Gold instruments.
- See a clinical protocol for canal preparation with the primary WaveOne Gold.
In this CE, Drs. Peet van der Vyver and Martin Vorster show how WaveOne reciprocating instruments provide clinicians with safety, simplicity, and superior results.
Drs. Peet van der Vyver and Martin Vorster discuss the clinical applications and guidelines of WaveOne® Gold reciprocating instruments

The WaveOne® nickel-titanium file system was introduced to the dental market in 2011. It was a pre-packaged, pre-sterilized, single-use system that was designed to shape root canal systems to a continuously tapering morphology (Webber, et al., 2011; van der Vyver, 2011). Recently, WaveOne® Gold, a new generation of reciprocating files, was launched. According to Webber (2015), these single-use shaping files offer the clinician more simplicity, safety, improved cutting efficiency, and mechanical properties compared to the previous generation of reciprocating instruments.
In this article, the authors will discuss the design features of the instruments and focus on the WaveOne Gold primary file. This primary file can be used in approximately 80%-85% of cases as a single file technique for root canal preparation. In part 2 of this series, we will discuss the management of larger diameter root canals systems, more challenging and curved root canal systems, and provide the reader with examples on when to use more than one WaveOne Gold file for canal preparation.
When conventional nickel-titanium instruments are rotated in root canals, they are subjected to structural fatigue that, if continued, will eventually lead to fracture (Sotokawa, 1988; Pruett, Clement, Carnes, 1997). Torsion and fatigue through flexure are the two main reasons for this failure (Serene, Adams, Saxena, 1995). Torsional fractures occur when the tip or any other part of the rotating instrument binds to the root canal walls, while the rest of the file keeps turning. Fracture due to flexural fatigue (bending stress) occurs when an instrument that has already been weakened by metal fatigue is placed under further stress. The instrument does not bind to the root canal walls but rotates freely until fracture of the instrument occurs at the point of maximum flexure (Gabel, et al., 1999; Sattapan, Palamara, Messer, 2000). The amount of bending stress imposed on an instrument depends on the anatomy of the root canal and is obviously greater in curved root canals (Pruett, Clement, Carnes, 1997).
The first study experimenting with an alternating movement was that of Yared in 2008, which used the ProTaper® F2 instrument (Dentsply Sirona) in a reciprocating movement (Yared, 2008). The alternating changes in direction of rotation would, in theory, reduce the number of cycles of the instrument and, therefore, reduce the cyclic fatigue on the instrument compared with that imposed when instruments are used in a consistent rotating motion (You, et al., 2010; Varela-Patiño, et al., 2010). The study showed great promise for the reduction of the number of instruments required in the cleaning and shaping sequence; in minimizing possible contamination; and alleviating operator anxiety of the possibility of instrument failure (Yared, 2008). Apart from these benefits, preparation time was shown to be faster than when using the same instrument in full rotation (You, et al., 2010). These findings were confirmed by Bürklein and Schäfer in 2012 when they compared Reciproc® (VDW) and WaveOne (Dentsply Sirona) functioning in reciprocating motion to Mtwo® (VDW) and ProTaper in conventional use (Bürklein, Schäfer, 2012).
Reciprocation motion
Instead of a rotary motion, the files work in a reverse “balanced force” cutting motion (Sotokawa, 1988) and are driven by a pre-programmed motor (X-Smart™ Plus motor fitted with 6:1 reducing handpiece) (Dentsply Sirona) or the new X-Smart™ IQ (Dentsply Sirona) endodontic motor fitted with a 8:1 reducing handpiece (paired to an iPad® mini) that is capable of turning the files in a back and forth “reciprocating” motion.
The counterclockwise (CCW) movement of 150 degrees is capable of advancing the instrument apically as the dentin on the root canal wall is engaged and cut. This movement is followed by a 30-degree clockwise (CW) movement, which ensures that the instrument disengages before excessive torsional stress is transferred onto the metal alloy and before the instrument can bind (taper lock) into the root canal. Three sequential reciprocating cycles will complete one whole reverse CCW rotation, and the repeated cutting and release process allows the instrument to advance apically into the root canal (Webber et al, 2011).
This unequal CW/CCW reciprocating motion of the WaveOne Gold system has the following advantages over continuous rotation systems:
- Binding of the instruments into the root canal dentin walls is less frequent, reducing torsional stress (Varela-Patiño, et al., 2008).
- The reduction of the number of cycles within the root canal during preparation results in less flexural stress on the instrument (Sattapan, Palamara, Messer, 2000).
- Improved safety, as the CCW disengaging angle is designed to be less than the elastic limit of the instrument (Ruddle, 2016).
- There is decreased risk of instrument fracture (Yared, 2008; Varela-Patiño, et al., 2008).
- It allows the file to easily progress toward working length without using potentially dangerous inward pressure (Yared, 2008; Ruddle, 2016).
- It enhances the augering of cutting debris out of the canal during canal preparation (Ruddle, 2016; De-Deus, et al., 2010).
Metallurgy and design features
The conventional WaveOne system was manufactured from M-Wire technology. M-Wire is prepared by a special thermal process, claimed to increase flexibility and resistance to cyclic fatigue (Gambarini, et al., 2008; Shen, et al., 2013). WaveOne Gold instruments are manufactured using a post-manufacturing thermal process whereby a new phase-transition point between martensite and austenite is identified to produce a file with superelastic nickel-titanium metal properties. This process gives the file a gold finish with improved mechanical characteristics. The WaveOne Gold primary file (Dentsply Sirona) is 50% more resistant to cyclic fatigue, 80% more flexible, and 23% more efficient than the conventional WaveOne primary instrument (Ruddle, 2016; Webber, 2015).





Why reciprocation?

Due to the superelastic properties of the new gold wire, the file may appear slightly curved when it is removed from a curved root canal because the metal demonstrates less memory compared to conventional nickel-titanium or M-Wire (Figure 1). The file can either be straightened out, or if it is placed back into a root canal, it will follow the natural shape of that canal (Webber, 2015). Another advantage of this reduced memory of the file is that in cases with difficult straight-line access, it is possible to slightly precurve the file, to allow easy placement into the canal orifices.
Conventional WaveOne instruments were characterized by different cross-sectional designs over the entire length of the working part of the instruments. In the tip region, the cross section presented radial lands, while in the middle part and near the shaft, the cross-sectional diameter changed from a modified triangular/convex cross section with radial lands to a neutral rake angle with a triangular/convex cross section (Bürklein, et al., 2012).
WaveOne Gold files are characterized with a parallelogram (with two 85-degree cutting edges) off-centered, cross section (Webber, 2015). According to Ruddle, this design limits the engagement between the file and the dentin to only one or two contact points at any given cross section. This will subsequently reduce taper lock and the screw-effect, improve safety and cutting efficiency, and provide more space around the instrument to remove debris coronally during canal preparation (Ruddle, 2016).
The newly designed files are also manufactured with an ogival, roundly tapered, and semi-active guiding tip to ensure that the file progresses safely along canals with a secured and confirmed reproducible glide path (Webber, 2015; Ruddle, 2016).
The WaveOne Gold single-file reciprocating system is available in four different file tip sizes in lengths of 21 mm, 25 mm, and 31 mm:
- WaveOne Gold small file (yellow ring) (Figure 2) — tip of the file is size ISO 20, and the first 3 mm of the file (D1- D3) has a continuous taper of 7%.
- WaveOne Gold primary file (red ring) (Figure 3) — tip of the file is size ISO 25, and the first 3 mm of the file (D1- D3) has a continuous taper of 7%.
- WaveOne Gold medium file (green ring) (Figure 4) — tip of the file is ISO 35, and the first 3 mm of the file (D1-D3) has a continuous taper of 6%.
- WaveOne Gold large file (white ring) (Figure 5) — tip of the file is ISO 45, and the first 3 mm of the file (D1-D3) has a continuous taper of 5%.
From D4-D16, each file demonstrates a progressively decreasing percentage tapered design to ensure more flexibility and to preserve more dentin in the body of the prepared root canal to ensure more conservative root canal preparations (Ruddle, 2016; Webber, 2015).
The WaveOne Gold files also have shortened 11-mm handles (Figure 6) that improve straight-line access into the posterior region of the mouth. It is color-coded (according to ISO size) with an expanding ABS ring after autoclaving to promote the philosophy of single use (Webber, 2015).
All of the previously mentioned product features produce a file system with improved mechanical and clinical benefits to ensure predictable root canal preparation. In the majority of cases, a single file can be used to complete root canal preparation with adequate resistance form to ensure exchange of irrigation solutions for adequate disinfection prior to root canal obturation in single or multiple root canal systems (Figure 7).
Clinical guidelines for the use of WaveOne Gold instruments
1. Create adequate access
It is always important to prepare an adequate access cavity that will ensure straight-line access into each root canal system after removal of all the pulp chamber contents. Ultrasonic instruments — e.g., Start-X ultrasonic instruments (Dentsply Sirona) — are very useful instruments to remove any pulp calcification and to refine the access cavity walls to improve straight-line access.
However, another characteristic of the new WaveOne Gold instruments are that the metal has less memory compared to conventional nickel-titanium or M-Wire instruments. It is therefore possible to slightly prebend the tip of the file to allow easy insertion into a secured canal orifice that fails to have complete straight-line access or in cases where patients present with a limited amount of mouth opening.
2. Select the correct WaveOne Gold file
The following guidelines can be used for WaveOne Gold file selection.
a. WaveOne Gold primary file (25/07) (Figure 3)
Any canal where a size 08 and 10 K-file has to be negotiated to working length, followed by preparation of a glide path or where a size 15 K-file fits loose in the canal to working length. This will usually include the majority of root canal systems with average length with moderate curvatures in mid-root and apical regions.
b. WaveOne Gold medium file (35/06) (Figure 4)
Any canal where a size 20 or 25 K-file fits loose in the canal and is not necessary to negotiate and prepare a glide path with smaller instruments. This will usually include larger diameter, relatively straight root canals. This file can also be used after the primary file if more shape is desired, or if it is felt that not enough infected dentin was removed from the canal.
c. WaveOne Gold large file (45/05) (Figure 5)
Any canal where a size 30 or 35 K-file fits loose in the canal and is not necessary to negotiate and prepare a glide path with smaller instruments. This will usually include larger diameter, relatively straight root canals. This file can also be used after the medium file if more shape is desired, or if it is felt that not enough infected dentin was removed from the canal.
d. WaveOne Gold small file (20/07) (Figure 2)
The small WaveOne Gold file is mainly used when the primary 25/07 file does not passively progress apically, or when the operator feels insecure with the primary file, after the canal was negotiated to patency and a glide path prepared. When this small file reaches working length, the clinician may accept the canal preparation or, alternatively, if more shape is required, to further enlarge the canal with the primary 25/07 file. The small file is then considered as a “bridge file” between the small and primary file (Ruddle, 2016).
However, in canals with severe apical curvatures, very long root canals or in canals where the glide path preparation was very challenging, the WaveOne Gold small file can be used to start root canal preparation with more safety. When this file reaches working length, the clinician may again accept the canal preparation or, alternatively, if more shape is required, further enlarge the canal with the primary 25/07 file.

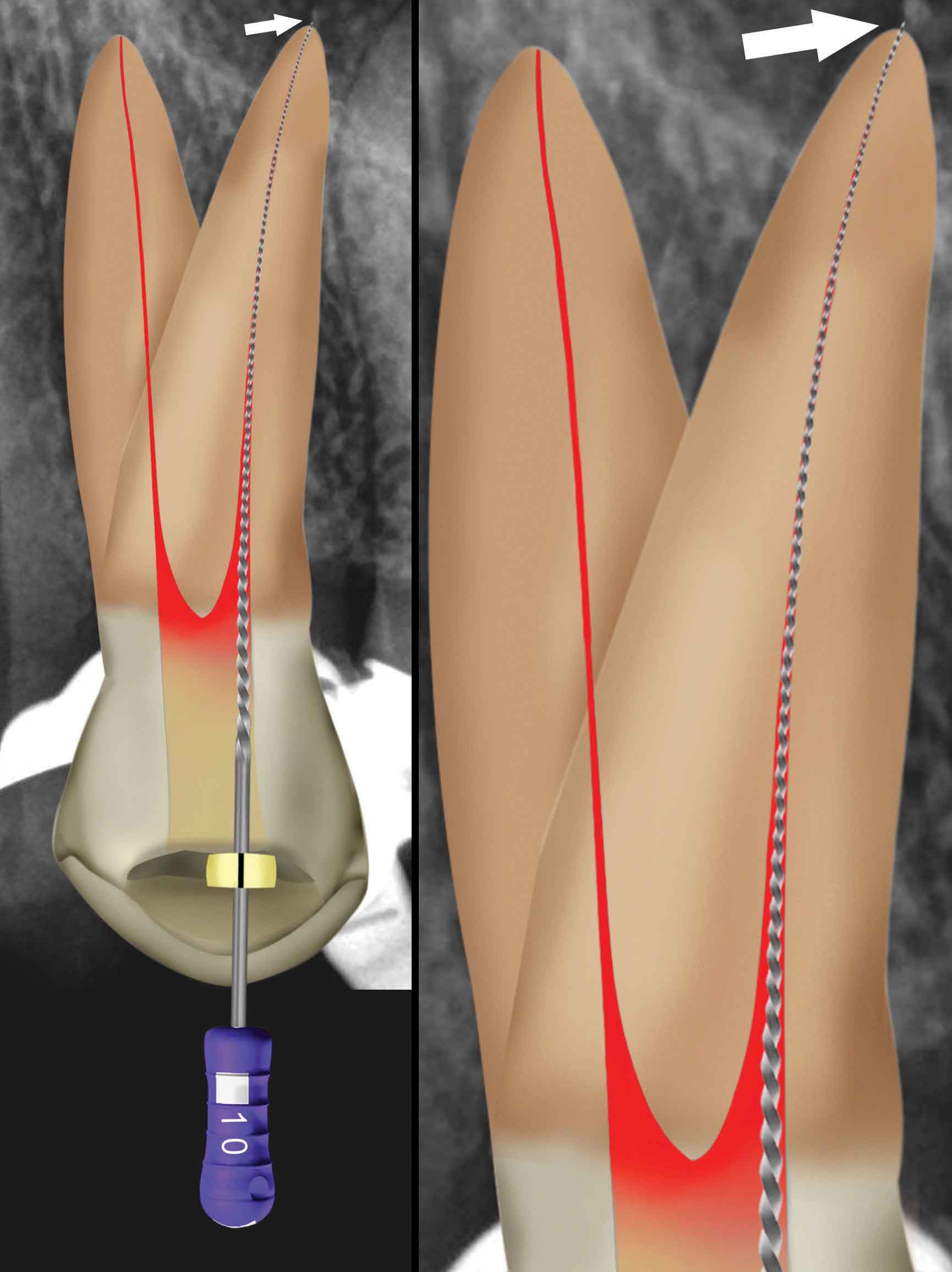


Figure 10: Periapical radiograph showing the position of the files during length determination — two size 10 K-files in buccal and palatal root canal (left) and Figure 11: Clinical confirmation of reproducible glide path: a super “loose” 10 K-file must able to travel 4 mm-5 mm to and from working length without any obstruction (right)


Clinical protocol for canal prep-aration with the primary WaveOne Gold file

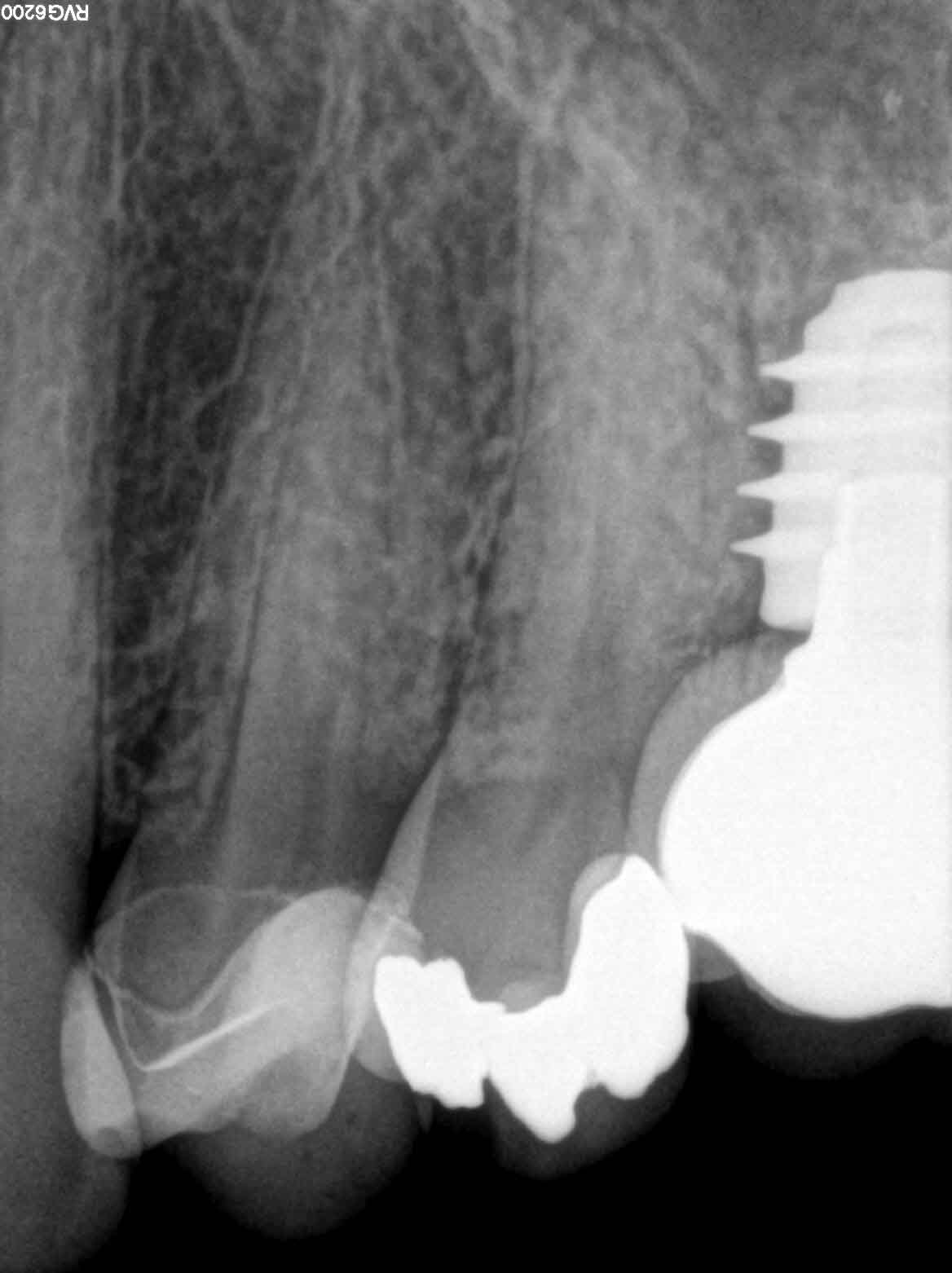
When we select the primary file for canal preparation, it is generally a canal where a size 08 and 10 K-file has to be negotiated to working length, followed by preparation of a glide path or where a size 15 K-file fits loose in the canal to working length. If we need to negotiate the canal and prepare a glide path, the authors would recommend the following protocol as outlined in the following example. The patient, a 40-year-old female presented with a nonvital right maxillary first premolar with decay under a previously placed composite restoration (Figure 8).

With an estimated working length obtained from a preoperative radiograph, a size 08 or 10 K-file is negotiated to patency in the presence of a viscous chelator. After the establishment of patency (Figure 9), a working length is determined (Figure 10), and the canal is ready for the preparation of a reproducible manual glide path (RMG), using manual stainless-steel instruments (van der Vyver, 2011). It is recommended to use size 08 or 10 K-files in a vertical in-and-out motion with an amplitude of 1 mm from working length, gradually increasing the amplitude to approximately 4 mm, as the irregularities are removed from the dentin wall (van der Vyver, 2011). A “super loose” size 10 K-file is the minimum requirement (Bürklein, et al., 2012; van der Vyver, 2011).
To confirm that a reproducible glide path is present, a size 10 K-file is taken to full working length. The file is withdrawn 1 mm and should be able to slide back to working length by using only light finger pressure. Thereafter, the file is withdrawn 2 mm and should be able to go to working length, using the same protocol. When the file can be withdrawn 4 mm-5 mm and slides back to working length, an RMG is confirmed (Figure 11). After the establishment of an RMG, it is recommended to enlarge the glide path further to create a macro glide path. The micro glide path can be expanded by using either the ProGlider® (Dentsply Sirona) (Figure 12) or WaveOne Gold Glider (Dentsply Sirona). Both are single file glide path instruments. The ProGlider is a rotating instrument with an ISO size 16 tip and 2% taper manufactured from M-Wire. The taper then progressively increases to 8.5% over the 18 mm of active cutting flutes. The WaveOne Gold Glider operates in a reciprocating motion with an ISO size 15 tip and 2% taper manufactured from gold wire. The taper then increases to 6% over the length of the active cutting flutes.

Canal preparation with the primary WaveOne Gold file

The authors suggest a controlled and disciplined way to ensure predictably cutting cycles without the risk of overstressing the file, reducing cutting efficiency, and reducing the risk of debris extrusion is to control the length of each cutting cycle. After glide path preparation (of all the canals), insert the primary file into the buccal or palatal root canal and record the initial depth of the file penetration by adjusting the rubber stop to a reference point on the cusp tip of the tooth (Figure 13 left). Remove the instrument from the root canal and record the length. Repeat the same procedure for the other canal and take an average of the measured length between the two canals. Move the rubber stop to a working length of 4 mm-6 mm (depending on your level of expertise) longer than the initial recorded length (Figure 13 middle).
The primary file in the presence of an irrigation solution (sodium hypochlorite, NaOCl), is allowed to passively advance inwards and to progress down the canal upon activation of the reciprocating motor. A brushing motion is only utilized in canals with irregular cross sections or to remove coronal interferences when necessary. The objective with the first cutting cycle will be only to cut with the instrument until the rubber stop reaches the cusp reference point (Figure 13 right), thereby ensuring that the operator knows that it is time to remove the instrument and clean the cutting debris from the flutes (Figure 14). After cleaning of the cutting flutes, it is advisable to inspect the cutting flutes for any visible distortion or unwinding of the flutes (Figure 15) before using the instrument again. After cleaning the flutes of the file, the first cutting cycle can be preformed in the buccal canal using the same protocol.
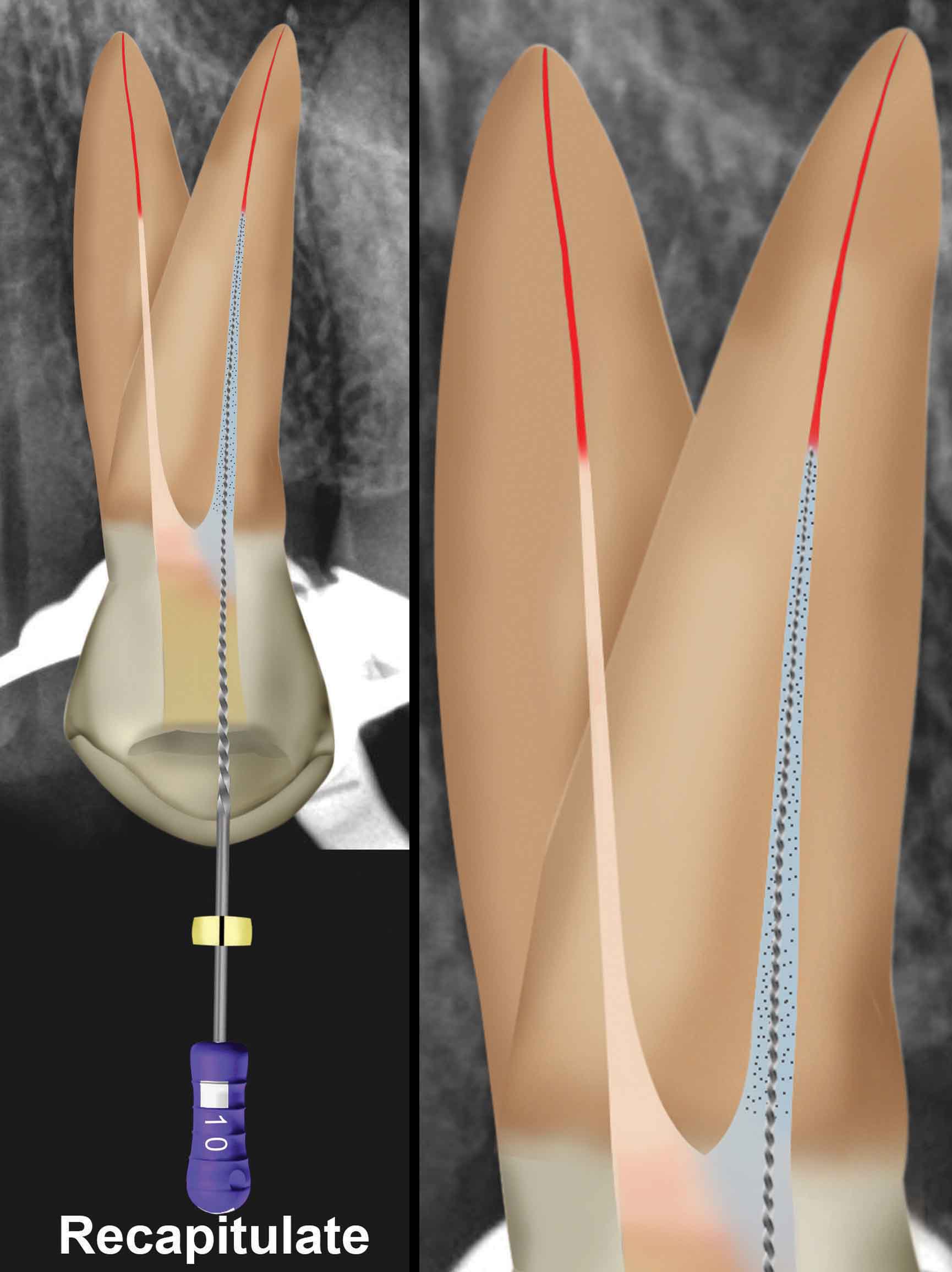
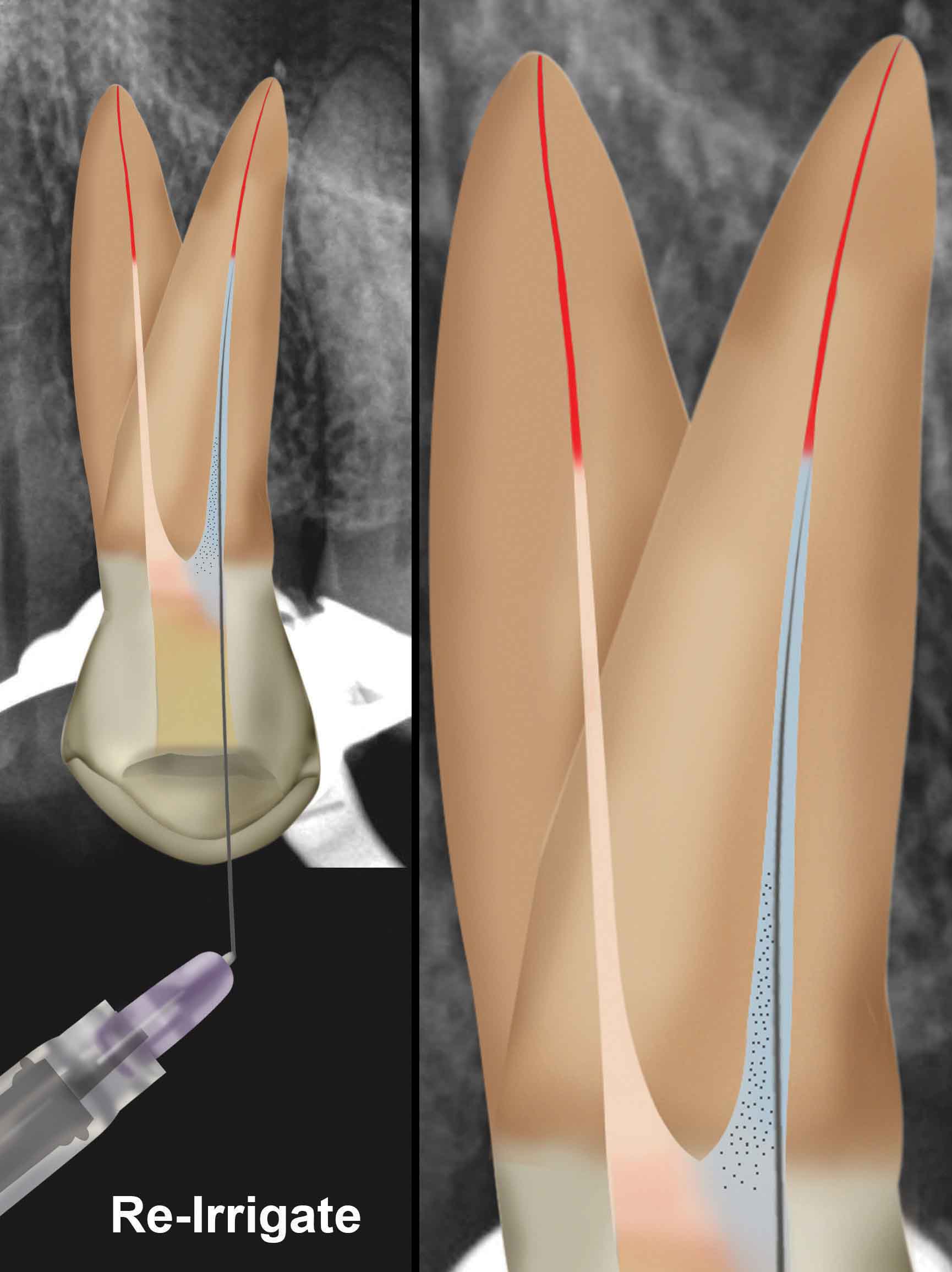
Before the next cutting cycle, it is recommended to also remove any loose and compacted debris from the root canal and that the glide path is still reproducible, and the canal is patent. This is achieved by dispensing an irrigation solution (NaOCl) into the root canal (Figure 16A), followed by inserting a 08 or 10 K-file, using a watch-wind motion (recapitulation) in the canal (Figure 16B), followed by a final irrigation step (irrigation-recapitulation-re-irrigation, IRR) (Figure 16C). The objective of recapitulation is to loosen up any compacted debris and move it back into solution before it is flushed out of the canal. The root canal and the instrument are now ready for the next cutting cycle.

The rubber stop on the instrument is again adjusted to a further 4 mm-6 mm longer or up to the point of the predetermined working length (Figure 17A). Again, the objective of the second cutting cycle will be to only cut with the instrument until the rubber stop reaches the cusp reference point. The same protocol is followed after each cutting cycle as outlined previously until predetermined working length of the root canal is reached (Figure 17B).
When the primary file tip reaches full working length, the file is withdrawn from the canal and inspected. Some articles recommend that if the apical 2 mm-3 mm of the flutes are filled with cutting debris, it would indicate that shaping in the apical part of the canal is adequate. If the flutes have no evidence of dentinal debris, it is advisable to continue shaping with the WaveOne gold medium and or WaveOne gold large file. Gauging the apical foramen with a corresponding nickel-titanium hand file is another alternative (Ruddle, 2016).
For example, if the final canal preparation was done with a primary 25/07 instrument, a size 25/02 nickel-titanium hand file (Dentsply Sirona) is fitted into the prepared root canal. If the tip of the file is snug at length, the final shape is confirmed, and a matching WaveOne Gold primary gutta-percha point (Dentsply Sirona), or a size 25 GuttaCore® Obturator (Dentsply Sirona) is used for cone fit or verification radiograph, prior to obturation. If the 25/02 nickel-titanium hand file is loose at length, or if it can be pushed past working length, it means that the apical foramen is larger than 0.25 mm. In these cases, it is recommended to gauge the apical foramen with a size 30/02 nickel-titanium hand file. If this instrument is snug at working length, the shape is confirmed to an ISO size 30. If the size 30/02 file is loose at length, then proceed to the medium WaveOne Gold instrument, or if necessary the large WaveOne Gold instrument using the same protocol as described previously.

In this clinical case, the tip of a size 25/02 nickel-titanium hand file fitted snug at working length in the buccal and palatal (Figure 18) canals, and matching WaveOne Gold primary gutta-percha points were placed and verified radiographically (Figure 19). The prepared canals filled with 17% EDTA and the solution activated for 1 minute with the EDDY™ Endo Irrigation Tip (VDW) driven by an airscaler (SONICflex™ LUX 2000L, KaVo) (Figure 20). Thereafter, final disinfection was achieved by activating 3.5% heated sodium hypochlorite for 3 minutes, again activated with the EDDY Endo Irrigation Tip.
The canals were dried with paper points and obturated using the gutta-percha points, Pulp Canal Sealer (Kerr) and the Calamus® Dual Obturation Unit (Dentsply Sirona). Figure 21 shows the final result after obturation.
The following case reports were all done using a single primary WaveOne Gold file for the root canal preparation to illustrate the simplicity, speed and superior results of the system.
Case report 1
The patient, a 31-year-old female, presented with a nonvital mandibular left first molar. Figure 22A shows the preoperative periapical radiograph, and Figure 22B the postoperative result after root canal preparation, irrigation, and obturation of the two mesial and one distal root canals, using a single WaveOne Gold 25/07 file.
Case report 2

The patient, a 52-year-old female, presented with irreversible pulpitis on her maxillary right first premolar. A preoperative periapical radiograph revealed a very deep, previously placed Class II composite restoration (Figure 23A). After access cavity preparation, three root canal systems were detected (two buccal and one palatal). All three root canals were prepared with a WaveOne Gold primary 25/07 file after glide path preparation using stainless steel K-files and a ProGlider. Figure 23B depicts the postoperative result after obturation of the root canals and placement of fiber post and composite core.
Case report 3

The patient, a 51-year-old female, presented with a nonvital maxillary left first molar restored with a porcelain-veneered crown. A preoperative periapical radiograph (Figure 24A) and CBCT scan revealed a conical root configuration.
After access cavity preparation, mesiobuccal, distobuccal, and palatal root canals were located, and a glide path preparation was done with stainless steel K-files and a ProGlider. Figure 24B illustrates the postoperative radiograph after the canals were prepared with a single WaveOne Gold primary file and the canals obturated.
Case report 4
The patient, a 51-year-old male, presented with a nonvital mandibular right canine. A preoperative periapical radiograph revealed a large root canal system in the coronal aspect of the tooth before the canal bifurcates (Figure 25A). A CBCT scan confirmed that there were two separate roots. Also visible on the radiograph is a plate from a previous osteotomy procedure 11 years ago, and at that time, the surgeon damaged the root of the mandibular second premolar. MTA was packed as an obturation material. An access cavity was prepared on the labial aspect of the tooth to provide straight-line access into the two root canal systems. After glide path preparation, the two root canals were prepared with the primary 25/07 WaveOne Gold file. After irrigation, two primary WaveOne Gold gutta-percha points were fitted (Figure 25B) and verified radiographically. Figure 15C shows the final result after root canal obturation and the access cavity closed with SDR® posterior bulk fill flowable base (Dentsply Sirona) and capped with a final layer of ceram.x® Sphere TEC™ one composite resin (Dentsply Sirona).
Case report 5
The patient, a 46-year-old female, presented with a nonvital maxillary left first molar. A preoperative periapical radiograph revealed that the tooth was treated previously with an emergency root canal treatment (Figure 26A). Four root canal systems, a mesiobuccal, a second mesiobuccal, distobuccal, and palatal root canals were located, and glide path preparation was done with stainless steel K-files and a ProGlider instrument. Figure 26B illustrates the postoperative radiograph after the four canals were prepared with a single WaveOne Gold primary file and the canals obturated. The palatal and distobuccal root canals were obturated with WaveOne Gold primary gutta-percha points and the two mesiobuccal root canals using two size 25 GuttaCore obturators.









Conclusions
- The design and metallurgy of the WaveOne Gold instruments provides the operator with improved cutting efficiency, flexibility, and nearly complete elimination of file fracture if the instruments are used single use
- In approximately 80%-85% of clinical cases, the clinician will need only the single primary WaveOne Gold file to complete canal instrumentation
- The single file shaping technique with the WaveOne Gold primary file, as illustrated in this article, provide clinicians with three distinct advantages: safety, simplicity, and superior results
Want to learn more about WaveOne instruments? Check out Dr. Peter Raftery’s article “Minimally invasive endodontics” here.
References
- Bürklein S, Hinschitza K, Dammaschke T, Schäfer E. Shaping ability and cleaning effectiveness of two single-file systems in severely curved root canals of extracted teeth: Reciproc and WaveOne versus Mtwo and ProTaper. Int Endod J. 2012;45(5):449-461.
- Bürklein S, Schäfer E. Apically extruded debris with reciprocating single-file and full-sequence rotary instrumentation systems. J Endod. 2012;38(6):850-852.
- De-Deus G, Brandão MC, Barino B, et al. Assessment of apically extruded debris produced by the single-file ProTaper F2 technique under reciprocating movement. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010;110(3):390-394.
- Gabel WP, Hoen M, Steiman HR, Pink FE, Dietz R. Effect of rotational speed on nickel-titanium file distortion. J Endod. 1999;25(11):752-754.
- Gambarini G, Grande NM, Plotino G, et al. Fatigue resistance of engine-driven rotary nickel-titanium instruments produced by new manufacturing methods. J Endod. 2008;34(8):1003-1005.
- Pruett JP, Clement DJ, Carnes DL. Cyclic fatigue testing of nickel-titanium endodontic instruments. J Endod. 1997;23(2):77-85.
- Ruddle CJ. Single-file shaping technique: achieving a gold medal result. Dent Today. 2016;35(1):98, 100, 102-103.
- Sattapan B, Palamara JE, Messer HH. Torque during canal instrumentation using rotary nickel-titanium files. J Endod. 2000;26(3):156-160.
- Serene TP, Adams JD, Saxena A. Nickel-titanium instruments: applications in endodontics. St. Louis, MO: Ishiyaku EuroAmerica; 1995.
- Shen Y, Zhou HM, Zheng YF, Peng B, Haapasalo M. Current challenges and concepts of the thermomechanical treatment of nickel-titanium instruments. J Endod. 2013;39(2):163-172.
- Sotokawa T. An analysis of clinical breakage of root canal instruments. J Endod. 1988;14(2):75-82.
- Van der Vyver PJ. WaveOne instruments: clinical application guidelines. Endodontic Practice. 2011; 45-54.
- Varela-Patiño P, Ibañez-Párraga A, Rivas-Mundiña B, et al. Alternating versus continuous rotation: a comparative study of the effect on instrument life. J Endod. 2010;36(1):157-159.
- Varela-Patiño P, Martín-Biedma B, Rodriguez-Nogueira J, et al. Fracture rate of nickel-titanium instruments using continuous versus alternating rotation. Endod Prac Today. 2008;2:193-197.
- Webber J. Shaping canals with confidence: WaveOne GOLD single-file reciprocating system. International Dentistry. 2015;6(3)6-17.
- Webber J, Machtou P, Pertot W, et al. The WaveOne single-file reciprocating system. Roots. 2011;1:28-33.
- Yared G. Canal preparation using only one Ni-Ti rotary instrument: preliminary observations. Int Endod J. 2008; 41(4):339-344.
- You SY, Bae KS, Baek SH, et al. Lifespan of one nickel-titanium rotary file with reciprocating motion in curved root canals. J Endod. 2010;36(12):1991-1994.
Stay Relevant With Endodontic Practice US
Join our email list for CE courses and webinars, articles and more..
