Shahriar A. Rassoulian, DMD; Shireen Sharif; and Sara Rodriguez describe root canal therapy with the Sonendo® GentleWave™ System
Abstract
 Introduction: This article suggests a novel approach to root canal therapy, the Sonendo® GentleWave™ System, which has shown an early healing response. This case provides details on a necrotic tooth treated with minimal shaping and the Multisonic Ultracleaning™ technology using the GentleWave System.
Introduction: This article suggests a novel approach to root canal therapy, the Sonendo® GentleWave™ System, which has shown an early healing response. This case provides details on a necrotic tooth treated with minimal shaping and the Multisonic Ultracleaning™ technology using the GentleWave System.
Methods: A patient was treated with the Sonendo GentleWave System after being referred for root canal therapy. The patient was followed for 9 months posttreatment with recalls every 3 months.
Results: The Multisonic UltraCleaning technique was successful in eliminating patient symptoms by the 3-month recall visit. The case suggests clear signs of healing in the periradicular region, as seen by a significant reduction in the size of the lesion at the 3-month recall.
Conclusion: The case describes radiographic and clinical outcomes associated with signs of early healing for a necrotic molar tooth treated with the novel Sonendo GentleWave System.
Introduction
 Healing time, and thereby reported success of root canal therapy, varies widely across the literature.1-4 Generally, most healing is reported to occur during the first year following the root canal treatment, although complete healing has been reported to take up to 4 or more years.4-7 When compiling the results of literature available for a composite radiographic and clinical endpoint to determine success, the approximate success rate for 1-year post root canal therapy is 68%-70%, while the success rate after 2 to 4 years rises to 80%-85%.
Healing time, and thereby reported success of root canal therapy, varies widely across the literature.1-4 Generally, most healing is reported to occur during the first year following the root canal treatment, although complete healing has been reported to take up to 4 or more years.4-7 When compiling the results of literature available for a composite radiographic and clinical endpoint to determine success, the approximate success rate for 1-year post root canal therapy is 68%-70%, while the success rate after 2 to 4 years rises to 80%-85%.
There are many factors that have been reported to affect the outcome of endodontic treatment. Overwhelmingly, the vast majority identifies the presence of a periradicular lesion as a major factor that can significantly reduce healing rates.1,4,8-17 Another commonly reported success predictor was the level of root filling. Sjögren reported that with adequate root filling within 2 mm of the apex, 94% of the cases showed normal periapical tissue at the follow-up examination.20 The number of roots treated and mid-treatment complications could also impact success rates.4,6,7,19,20 These factors may be the reason why the overall success rates seen in our literature review is 68%-70% at 12 months.
This case report provides details on a novel root canal therapy, the Sonendo GentleWave™ System’s Multisonic UltraCleaning™. The Sonendo GentleWave System introduces a novel method for cleaning root canals that may be safer, less invasive, and more efficient. The Sonendo GentleWave System is designed to conserve the natural tooth structure and minimize procedural difficulties and safety concerns. This case report describes the technique utilized and is supported by radiographic imaging.
Technique
A new technology, termed GentleWave™ System (Sonendo, Inc., Laguna Hills, California) has been developed to clean the root canal system with minimal instrumentation of the root canals.21 The GentleWave™ System consists of a console and a handpiece (Figure 1). During the treatment, and after accessing the pulp chamber, the tip of the handpiece is placed within the pulp chamber of an accessed molar tooth, cleaning the entire root canal system simultaneously. This necessitates only minimal or even no instrumentation of the root canals. The technology employs various phenomena, including a strong hydrodynamic cavitation cloud to generate a broad spectrum of sound waves, multisonic energy, which travels through a degassed fluid and into the entire root canal system. Degassed fluid refers to the treatment fluid with reduced amount of dissolved gas. This optimizes the delivery of energy throughout the root canal system, e.g., multisonic energy and fluid dynamics. Additional descriptions on the technology and its mechanism of action have been described in a recent study.22 It was demonstrated that the tissue dissolution efficacy of the GentleWave™ by far exceeds that of all the conventional irrigation systems used with sodium hypochlorite (NaOCl), including ultrasonic irrigation.
History
A 29-year-old female patient with Type I diabetes mellitus presented to the dental office with a complaint of pain on the upper right side of the oral cavity. The rest of the patient’s medical history was non-contributory.
Diagnosis
Upon arrival at the endodontic clinic 1 month later, clinical and radiographic examination was performed. The clinical examination revealed the right maxillary first molar (No. 3) with a fractured amalgam filling. Extensive occlusal and lingual caries were present with localized swelling and redness on the buccal aspect of the tooth. Periodontal probing revealed a deep 5-mm periodontal pocket distally. Vitality testing with Endo-Ice® (Coltene/Whaledent) revealed a negative response to cold. The tooth presented with no mobility, severe tenderness to vertical percussion, and moderate pain to palpation. Radiographic examination revealed widening of the periodontal ligament space around the mesiobuccal root and a large radiolucent lesion with defined borders associated with the palatal root. From the results obtained by clinical and radiographic examination, the subject tooth was diagnosed with pulpal necrosis and symptomatic apical periodontitis.
Treatment
After thorough diagnostic testing and evaluation of both presenting and history of symptoms confirming the need for a root canal therapy, the tooth was treated with a standardized root canal therapy protocol. Standard anesthetic technique and medication were utilized throughout the procedure. After rubber dam application, old restoration, and caries removal, conservative straight-line access was performed. Coronal flaring or enlargement was not performed in order to conserve tooth structure. Patency to the apical foramen was confirmed with K-type hand files (No. 10.02 and No. 15.02). The canals were instrumented to the smallest size file that bound at the apex. For the mesiobuccal and distobuccal canals, hand files to size 20.02 were utilized followed by standard NiTi rotary hand files to size 20.04. The mesiobuccal 2 canal was instrumented utilizing hand files to size 15.02 and final NiTi rotary file size 15.04, whereas the palatal canal was instrumented to a final NiTi rotary file size 40.06.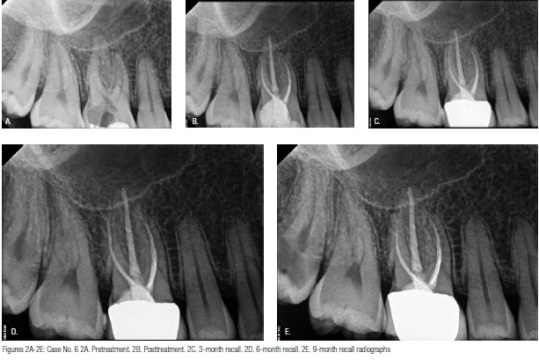 After minimal instrumentation, the Sonendo GentleWave System, which uses a Multisonic UltraCleaning Technique with sodium hypochlorite (NaOCl) (3%) and ethylenediaminetetraacetic acid (EDTA) (8%), was then utilized to remove debris and smear layer from all canals simultaneously. Each canal was then dried with paper points. The tooth was then obturated with single cone or warm vertical obturation using gutta percha and AH Plus® (Dentsply) sealer. The mesiobuccal and distobuccal canals were obturated with a single cone obturation technique due to the minimal instrumentation, while the palatal canal was obturated using warm vertical compaction. A palatal apical delta was visible post-obturation.
After minimal instrumentation, the Sonendo GentleWave System, which uses a Multisonic UltraCleaning Technique with sodium hypochlorite (NaOCl) (3%) and ethylenediaminetetraacetic acid (EDTA) (8%), was then utilized to remove debris and smear layer from all canals simultaneously. Each canal was then dried with paper points. The tooth was then obturated with single cone or warm vertical obturation using gutta percha and AH Plus® (Dentsply) sealer. The mesiobuccal and distobuccal canals were obturated with a single cone obturation technique due to the minimal instrumentation, while the palatal canal was obturated using warm vertical compaction. A palatal apical delta was visible post-obturation.
The pulp chamber floor was sealed with a resin-based filling material, and the tooth was restored with composite. After this single visit treatment, the patient returned to the endodontist for recalls every 3 months.
Outcome
At the 3-month recall, the tooth was asymptomatic and showed signs of healing. The patient did not report any pain. Radiographically, there was a marked reduction of the periapical radiolucency associated with the mesiobuccal and palatal roots.
At 6 months, the tooth remained asymptomatic with no pain reported by the patient. Clinical and radiographic examination confirmed the presence of periradicular healing that was initially seen at 3 months.
At 9 months, there were no remarkable changes clinically or radiographically, confirming the success of endodontic treatment.
Discussion
Clear indication of periapical healing has not typically been reported as early as at the 3-month time point. According to the literature, at 6 months, healing rates are at 62%, reaching only about 69% at the 12-month recall.23, 24 In review of this case report for a tooth treated with the Sonendo GentleWave System, early signs of healing were seen at the 3-month recall visit.
This case report illustrates the possibilities for the novel technique in endodontics, although long-term recall and a larger sample size are needed to confirm. Future studies are planned to show additional healing results after treatment with the Sonendo GentleWave System.
Acknowledgments
Supported and start-up funds were provided by Sonendo®, Inc. Sonendo was the study sponsor for the PURE study. The first author (S.R., DMD) serves as a consultant for Sonendo, Inc. The two other authors are employees of Sonendo, Inc.
References
Ng YL, Mann V, Rahbaran S, Lewsey J, Gulabivala, K. Outcome of primary root canal treatment: systematic review of the literature — Part 2. Influence of clinical factors. Int Endod J. 2008;41(1):6-31.
Torabinejad M, Anderson P., Bader J, Brown LJ, Chen LH, Goodacre CJ, Kattadiyil MT, Kutsenko D, Lozada J, Patel R, Petersen F, Puterman I, White SN.. Outcomes of root canal treatment and restoration, implant-supported single crowns, fixed partial dentures, and extraction without replacement: a systematic review. J Prosthet Dent. 2007;98(4):285-311.
Weiger, R., Axmann-Krcmar, D., Lost, C. Prognosis of conventional root canal treatment reconsidered. Endod Dent Traumatol. 1998;14(1):1-9.
de Chevigny C, Dao TT, Basrani BR, Marquis V, Farzaneh M, Abitbol S, Friedman S. Treatment outcome in endodontics: the Toronto study — phase 4: initial treatment. J Endod. 2008;34(3):258-263.
Friedman S, Abitbol S, Lawrence, HP. Treatment outcome in endodontics: the Toronto Study. Phase 1: initial treatment. J Endod. 2003;29(12):787-793.
Farzaneh M, Abitbol S, Lawrence HP, Friedman S. Treatment outcome in endodontics — the Toronto Study. Phase II: initial treatment. J Endod. 2004;30(5):302-309.
Marquis VL, Dao T, Farzaneh M, Abitbol S, Friedman S. Treatment outcome in endodontics: the Toronto Study. Phase III: initial treatment. J Endod. 2006;32(4):299-306.
Penesis VA, Fitzgerald PI, Fayad MI, Wenckus CS, BeGole EA, Johnson BR. Outcome of one-visit and two-visit endodontic treatment of necrotic teeth with apical periodontitis: a randomized controlled trial with one-year evaluation. J Endod. 2008;34(3):251-257.
Huumonen S, Lenander-Lumikari M, Sigurdsson A, Orstavik D. Healing of apical periodontitis after endodontic treatment: a comparison between a silicone-based and a zinc oxide-eugenol-based sealer. Int Endod J. 2003;36(4):296-301.
Spili P, Parashos P, Messer HH. The impact of instrument fracture on outcome of endodontic treatment. J Endod. 2005;31(12):845-850.
Zmener O, Pameijer CH. Clinical and radiographical evaluation of a resin-based root canal sealer: a 5-year follow-up. J Endod. 2007; 33(6):676-679.
Farzaneh M, Abitbol S, Lawrence HP, Friedman S. Treatment outcome in endodontics — the Toronto Study. Phase II: initial treatment. J Endod. 2004;30(5):302-309.
Cotton TP, Schindler WG, Schwartz SA, Watson WR, Hargreaves KM. A retrospective study comparing clinical outcomes after obturation with Resilon/Epiphany or Gutta-Percha/Kerr sealer. J Endod. 2008;34(7):789-797.
Hoskinson SE, Ng YL, Hoskinson AE, Moles DR, Gulabivala K. A retrospective comparison of outcome of root canal treatment using two different protocols. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2002;93(6):705-715.
McGuigan MB, Louca C, Duncan HF. The impact of fractured endodontic instruments on treatment outcome. Br Dent J. 2013;214(6):285-289.
Sjogren U, Hagglund B, Sundqvist G, Wing K. Factors affecting the long-term results of endodontic treatment. J Endod. 1990;16(10):498-504.
Heling B, Tamshe A. Evaluation of the success of endodontically treated teeth. Oral Surg Oral Med Oral Pathol. 1970; 30(4): 533-536.
Sjogren U, Hagglund B, Sundqvist G, Wing K. Factors affecting the long-term results of endodontic treatment. J Endod. 1990;16(10):498-504.
Kerekes K, Tronstad L. Long-term results of endodontic treatment performed with a standardized technique. J Endod. 1979;5(3):83-90.
Swartz DB, Skidmore AE, Griffin JA Jr. Twenty years of endodontic success and failure. J Endod. 1983;9(5):198-202.
Sonendo, Inc. www.sonendo.com. Accessed February 17, 2015.
Haapasalo M, Wang Z, Shen Y, Curtis A, Patel P, Khakpour M. Tissue Dissolution by a novel multisonic ultracleaning system and sodium hypochlorite. J Endod. 2014;40(8):1178-1181.
Martins MR, Carvalho MF, Vaz IP, Capelas JA, Martins MA, Gutknecht N. Efficacy of Er,Cr:YSGG laser with endodontical radial firing tips on the outcome of endodontic treatment: blind randomized controlled clinical trial with six-month evaluation. Lasers Med Sci. 2013;28(4):1049-1055.
Saini HR, Tewari S, Sangwan P, Duhan J, Gupta A. Effect of different apical preparation sizes on outcome of primary endodontic treatment: a randomized controlled trial. J Endod. 2012;38(10):1309-1315.
Stay Relevant With Endodontic Practice US
Join our email list for CE courses and webinars, articles and more..
