Drs. Clovis Monteiro Bramante, Murilo Priori Alcalde, Pablo Andrés Amoroso-Silva, Alexandre Silva Bramante, Helberth Gonzalis Giraldo, Rodrigo Ricci Vivan, and Marco Antonio Hungaro Duarte discuss possible anatomical variations that can be of consequence even in those teeth considered as less complex
Abstract
Introduction and objective
To describe a detailed analysis of the internal anatomy of an extracted maxillary central incisor with a rare anatomical variation, containing three roots and three canals using micro-computed tomography (CT).
Methods
The tooth was scanned using a micro-CT device and analyzed at 1 mm, 2 mm, and 3 mm from the apex, and cervical and middle-third of the root were selected. A quantitative analysis of the canal, roundness, and major and minor diameters was performed.
Results
The tooth’s crown had normal morphological characteristics but with grooves in the buccal aspects and in both the proximal aspects that started from the cemento-enamel junction and advanced towards the apical direction. At the cervical portion, a single wide canal was observed. In the middle-third of the root, the main canal bifurcated into a mesial and distal canal. The distal canal was oval shaped with a large major diameter, and the mesial canal presented lower values of major and minor diameters and a more rounded canal then the distal canal. At the apical region, a new bifurcation of the distal canal occurred giving rise to a palatal root, which was approximately 2 mm longer than the distobuccal root with similar morphometric measurements.
Conclusions
It is important that clinicians be aware of possible anatomical variations even in those teeth considered as less complex such as the one presented in this report. Furthermore, the radiographic examination did not provide anatomical details, which could be improved using other imaging diagnostic tools, such as cone beam CT.
Introduction
Knowledge regarding dental anatomy is an important prerequisite for successful endodontic treatment,1 which includes understanding the normal morphology of the root canal along with its anatomical variations that are encountered in clinical practice,2,3 thereby minimizing operative procedure errors, which can interfere with the success rate of endodontic treatments.1
Moreover, the internal root canal anatomy of anterior teeth is currently well established in the literature with numerous studies reporting the incidence of the number of roots and root canals of each dental group.4-9 Regarding the maxillary incisors, these teeth almost always possess a single root canal and a less complex internal anatomy. However, the presence of the two canals has been reported with a low variation percentage between 2% and 4% and may include the presence of two root canals in a single root or two root canals in two separate roots.5,6,10,11,12,13
Although the incidence of maxillary central incisors with two root canals is considered low, the literature contains many case reports.14-18 Furthermore, there are reports of maxillary central incisors with three root canals and one root,19,20 two roots and three canals,21 and four canals in one root.22
To date, there are no reports in the literature regarding maxillary central incisors presenting with three roots and three canals. This report aimed to provide a detailed analysis of the internal anatomy of an extracted maxillary central incisor containing three roots and three canals using micro-computed tomography (CT).
Methods
A maxillary central incisor was donated by a student from the Dental School of the Santa Maria Catholic University located in Arequipa, Peru. There was no possibility of obtaining an accurate case history because the student was unaware of the origin of the tooth.
Macroscopically, the tooth showed a crown with normal morphological characteristics in the buccal, palatal, and proximal aspects and within the average patterns of measurement for this tooth group. On the buccal aspect of the crown, a discreet groove was observed in the cervical region extending toward the buccal aspect of the root, thereby becoming more pronounced in the apical region where the bifurcation of the buccal roots occurred. Two roots in the buccal aspect and one in the palatal were observed. Both buccal roots exhibited a slight apical curvature toward the mesial side.
The palatal root was approximately 2 mm longer than the buccal roots and exhibited a severe curvature to the distobuccal direction in the apical portion of the root. Furthermore, in both, the proximal sides two radicular grooves were observed that started from the cementoenamel junction (Figure 1). During the radiographic examination, it was possible to observe a wide and single canal in the mesiodistal direction and flattened in the buccal-palatal direction until the middle-third where three root canals were observed (Figure 2).

Figure 1: Maxillary central incisor images. 1A. The buccal surface of the central incisor where it is possible to observe a pronounced groove that begins in the middle of the tooth crown, extending to the root in the apical direction where the bifurca-tion occurs. 1B. Proximal view, that shows a severe curvature towards the buccal direction of the palatal root. 1C. Palatal view

Figure 2: 1A. Radiographic image of the buccal aspect (left) and axial micro-CT image (right) of the maxillary central incisor, showing the internal anatomy with two buccal canals. 2B. Proximal view of the radiographic image (left) and sagittal view of the micro-CT showing the internal anatomy of the palatal canal
Micro-CT examination
For a more precise examination of the internal anatomy of this tooth, a micro-CT device Skyscan 1174 (Bruker-microCT, Kontich, Belgium) with the following parameters: 50 kV, 800 mA, 3600 of rotation, and an isotropic resolution of 19.6 mm was used to analyze the tooth. The image of the specimen was reconstructed using the NRecon v.1.6.3 software (Bruker-microCT) that provided axial cross sections of the inner structures of the roots in the bitmap format. The three-dimensional model was reconstructed using the automatic segmentation and surface modeling CTAn v.1.12 software (Bruker-microCT; Figure 3).
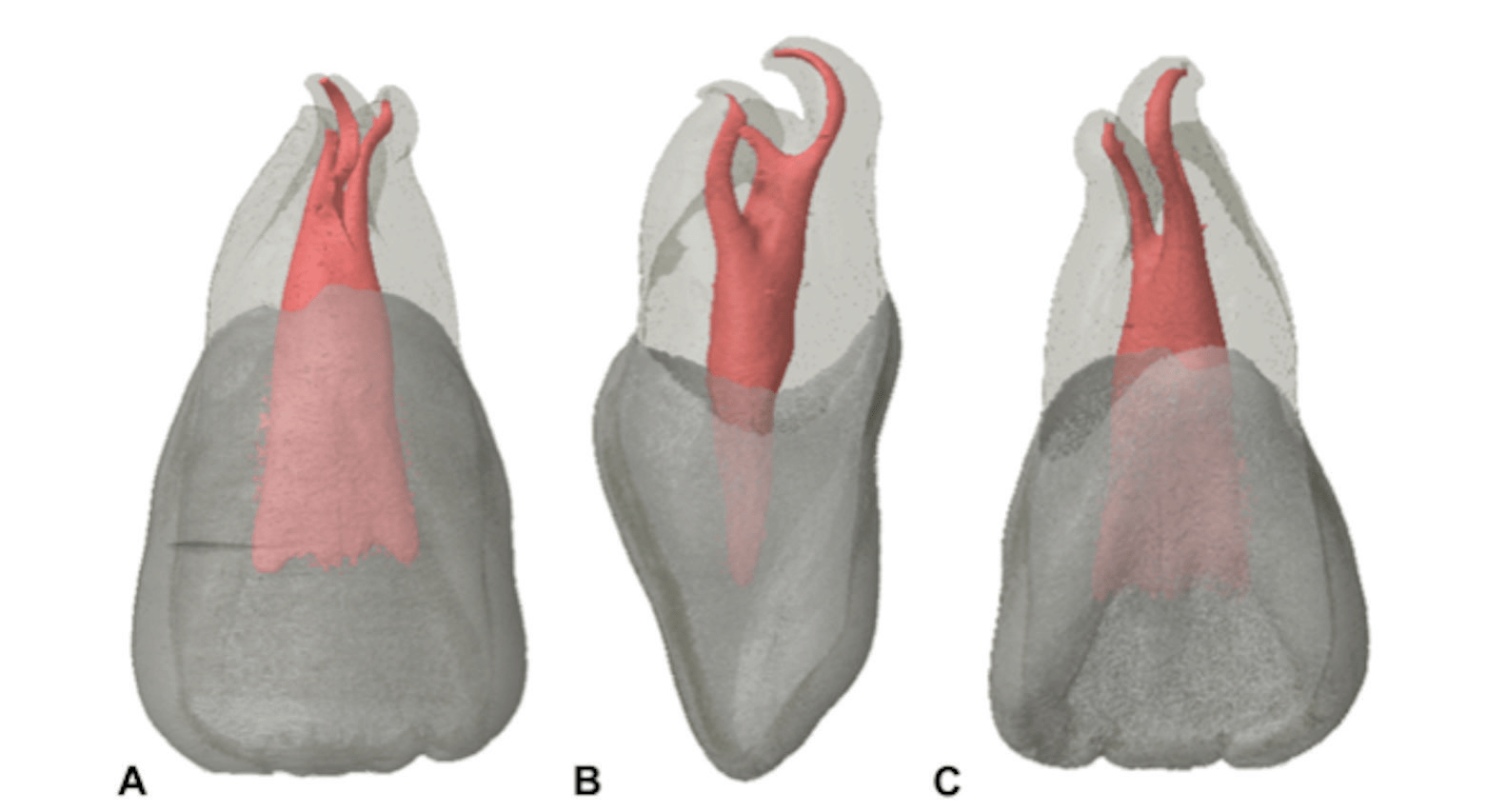
Figure 3: Micro-CT reconstruction of the internal and external anatomy of the MCI: 3A. buccal, 3B. proximal, and 3C. palatal view
Furthermore, two-dimensional cross sections that were taken at 1 mm, 2 mm, and 3 mm from the apex, and from the cervical and middle-third of the root were selected. Using the CTAn and data viewing software (Bruker-microCT), quantitative analysis of the canal, roundness, and major and minor diameters were performed. Figure 4 shows the morphometric data obtained in the micro-CT analysis. At the cervical portion, a single wide canal was observed. In the middle-third of the root, the main canal bifurcated into a mesial and distal canal. The distal canal was oval shaped with a large major diameter (1.72 mm), and the mesial canal presented with lower values of major and minor diameters and was more rounded than the distal canal. At the 3-mm and 2-mm sections, morphological canal characteristics similar to the ones of the middle-third section were observed.
At the apical region, a new bifurcation of the distal canal occurred giving origin to a palatal root, which was approximately 2 mm longer than the distobuccal root. In the cross section at 1 mm from the apex, the distobuccal and palatal canals had similar measurements. Contrary, the mesiobuccal canal had lower values of major and minor diameters and an oval-shaped canal.
Discussion
The anatomy of the maxillary central incisor is considered simple, containing a single root with a single canal in most cases. Anatomical variations of these teeth with more than one canal or root have been reported.16,17 However, the majority of these case reports are usually associated with some morphological abnormalities such as macrodontia, fusion, or germination, and dens in dens.23-26 Godim, et al.,27 published a case report of a central incisor with normal morphology containing three canals but only two roots. In our case, the three-rooted maxillary central incisor with three separate canals was not associated with any morphological abnormalities, which probably makes this case a very rare occurrence.
On observation of the extracted tooth, the crown was intact without any signs of decay or trauma and contained various radicular grooves, one on the vestibular portion and two at the proximal portions of the root. These may indicate that the cause of extraction originated from a periodontal problem, leading to a periodontal pocket and the loss of its supporting tissue.
The maxillary incisors may be affected by the presence of a palatogingival groove with major occurrence in lateral incisors, which can lead to periodontal problems and an association with endodontic problems.28,29 Although it is rare, radicular grooves can occur in the buccal root region 27,30 as was observed in this case. Such cases often require a multidisciplinary approach for restoring the periodontal tissue through periodontal and endodontic treatment.29
Micro-CT analysis revealed larger apical diameters in the palatal (0.67 mm) and distobuccal (0.60 mm) canals at 1 mm from the apex and lower values for the mesiobuccal canals (Figure 4). However, a previous study reported that the largest diameter at 1 mm from the apex in a maxillary central incisor was 0.3 mm–0.45-mm31 lower than the ones encountered in this report. Furthermore, because it occurs in a three-rooted tooth, the palatal canal presented the larger apical diameters.
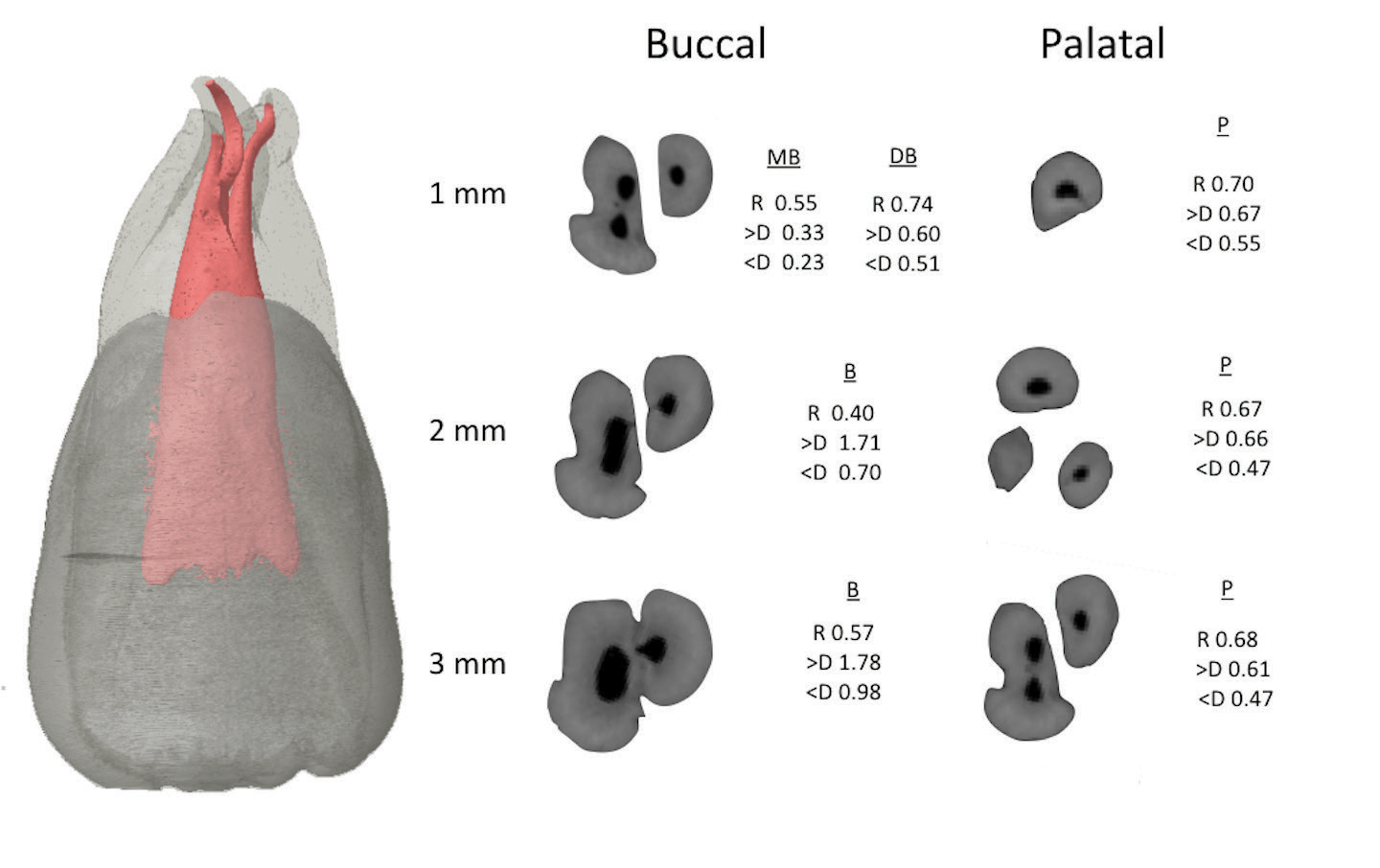
Figure 4: Morphometric values of roundness (R), major diameter (>D) and minor diameter (<D) of the different cross sections analyzed in the apical third from the buccal and palatal roots
The use of micro-CT technology enabled a precise evaluation of the internal tooth anatomy, in which it was possible to observe with more precision the anatomical variation of this maxillary central incisor with three roots and the exact point of bifurcation and trifurcation of the canals. These characteristics are important because in a conventional radiographic image, it would be difficult to observe the anatomical variations in such a detailed manner (Figure 2). In cases with a complex anatomy, the use of cone beam computed tomography (CBCT) could be used for a more precise evaluation of teeth with anatomical variations before endodontic treatment.32
Conclusions
It is important that clinicians be aware of possible anatomical variations even in those teeth considered as less complex such as the one presented in this report. Therefore, it is essential to implement radiographic or other imaging methods, such as CBCT, for an accurate diagnosis and a more predictable treatment of such cases.
- Vertucci FJ. Root canal morphology and its relationship to endodontic procedures. Endod Topics. 2005;10(1):3-29.
- Cantatore G, Berutti E, Castellucci A. Missed anatomy: frequency and clinical impact. Endod Topics. 2006; 5(1):3-31.
- Ahmed HM, Abbott PV. Accessory roots in maxillary molar teeth: a review and endodontic considerations. Aust Dent J. 2012;57(2):123-131.
- Vertucci FJ. Root canal anatomy of the mandibular anterior teeth. J Am Dent Assoc. 1974;89(2):369-371.
- Vertucci FJ. Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol. 1984;58(5):589-599.
- Pineda F, Kuttler Y. Mesiodistal and buccolingual roentgenographic investigation of 7,275 root canals. Oral Surg Oral Med Oral Pathol. 1972;33(1):101-110.
- Han T, Ma Y, Yang L, Chen X, Zhang X, Wang Y. A study of the root canal morphology of mandibular anterior teeth using cone-beam computed tomography in a Chinese subpopulation. J Endod. 2014;40(9):1309-1314.
- Milanezi de Almeida M, Bernardineli N, Ordinola-Zapata R, et al. Micro-computed tomography analysis of the root canal anatomy and prevalence of oval canals in mandibular incisors. J Endod. 2013;39(12):1529-1533.
- de Silva EJ, de Castro RW, Nejaim Y, et al. Evaluation of root canal configuration of maxillary and mandibular anterior teeth using cone beam computed tomography: An in-vivo study. Quintessence Int. 2016;47(1):19-24.
- Caliskan MK, Pehlivan Y, Sepetçioğlu F, Türkün M, Tuncer SS. Root canal morphology of human permanent teeth in a Turkish population. J Endod. 1995;21(4):200-204.
- Sert S, Bayirli GS. Evaluation of the root canal configurations of the mandibular and maxillary permanent teeth by gender in the Turkish population. J Endod. 2004;30(6):391-398.
- Rahimi S, Shahi S, Yavari HR, Reyhani MF, Ebrahimi ME, Rajabi E. A stereomicroscopy study of root apices of human maxillary central incisors and mandibular second premolars in an Iranian population. J Oral Sci. 2009;51(3):411-415.
- Calvert G. Maxillary central incisor with type V canal morphology: case report and literature review. J Endod. 2014;40(10):1684-1687.
- Michanowicz AE, Michanowicz JP, Ardila J, Posada A. Apical surgery on a two-rooted maxillary central incisor. J Endod. 1990;16(9):454-455.
- Lambruschini GM, Camps J. A two-rooted maxillary central incisor with a normal clinical crown. J Endod. 1993;19(2):95-96.
- González-Plata-R R, González-Plata-E W. Conventional and surgical treatment of a two-rooted maxillary central incisor. J Endod. 2003;29(6):422-424.
- Rao Genovese F, Marsico EM. Maxillary central incisor with two roots: a case report. J Endod. 2003;29(3):220-221.
- Lin WC, Yang SF, Pai SF. Nonsurgical endodontic treatment of a two-rooted maxillary central incisor. J Endod. 2006;32(5):478-481.
- Zaitoun H, Mackie IC. Management of a non-vital central incisor tooth with three root canals. Dent Update. 2004;31(3):142-144.
- Sheikh-Nezami M, Mokhber N. Endodontic treatment of a maxillary central incisor with three root canals. J Oral Sci. 2007;49(3):245-247.
- Mangani F, Ruddle CJ. Endodontic treatment of a “very particular” maxillary central incisor. J Endod. 1994;20(11):560-561.
- Aznar Portoles C, Moinzadeh AT, Shemesh H. A Central Incisor with 4 Independent Root Canals: A Case Report. J Endod. 2015;41(11):1903-1906.
- Oehlers FA. Dens invaginatus (dilated composite odontome). I. Variations of the invagination process and associated anterior crown forms. Oral Surg Oral Med Oral Pathol. 1957;10(12):1302-1316.
- Pereira AJ, Fidel RA, Fidel SR. Maxillary lateral incisor with two root canals: fusion, gemination or dens invaginatus? Braz Dent J . 2000;11(2):141-146.
- Alani A, Bishop K. Dens invaginatus. Part 1: classification, prevalence and aetiology. Int Endod J. 2008;41(12):1123-1136.
- Steinbock N, Wigler R, Kaufman AY, Lin S, Abu-El Naaj I, Aizenbud D. Fusion of central incisors with supernumerary teeth: A 10-year follow-up of multidisciplinary treatment. J Endod. 2014;40(7):1020-1024.
- Gondim E, Setzer F, Zingg P, Karabucak B. A maxillary central incisor with three root canals: a case report. J Endod. 2004; 35(10):1445-1447.
- Lara VS, Consolaro A, Bruce RS. Macroscopic and microscopic analysis of the palato-gingival groove. J Endod. 2000;26(6):345-350.
- Schwartz SA, Koch MA, Deas DE, Powell CA. Combined endodontic-periodontic treatment of a palatal groove: a case report. J Endod. 2006;32(6):573-578.
- Kerezoudis NP, Siskos GJ, Tsatsas V. Bilateral buccal radicular groove in maxillary incisors: case report. Int Endod J. 2007;36(12):898-906.
- Kerekes K, Tronstad L. Morphometric observations on root canals of human anterior teeth. J Endod. 1977;3(1):24-29.
- Levin A, Shemesh A, Katzenell V, Gottlieb A, Ben Itzhak J, Solomonov M. Use of Cone-beam Computed Tomography during Retreatment of a 2-rooted Maxillary Central Incisor: Case Report of a Complex Diagnosis and Treatment. J Endod. 2015;41(12):2064-2067.
Stay Relevant With Endodontic Practice US
Join our email list for CE courses and webinars, articles and more..
