Editor’s intro: Dr. Jorge Alberdi delves into correct endodontic and restorative diagnosis and how this can lead to successful tooth conservation.
Dr. Jorge Alberdi highlights the importance of endodontic retreatment for tooth conservation
Abstract
Endodontic retreatment is carried out in cases that previous endodontic therapies failed. The main cause of treatment failure is bacterial persistence within the root canal or coronal leakage after treatment. The key factor to achieving success should be to evaluate whether retreatment is viable from a pathological and restorative point of view. The literature reports a success rate ranging from 80% to 88% for endodontic retreatment; thus, it is a procedure with a predictable prognosis when well performed and, essentially, when there is a correct diagnosis. Prognosis will be affected by the type of previous treatment received by the tooth. Numerous technologies such as operative microscope, CBCT, and ultrasound are available to help execute the different procedures that could demand this therapy. Overall, clinical procedures include crown removal and/or access through the crown; removal of pins or posts and other core materials; removal of gutta percha, silver cones, pastes, and in some cases, even separated instruments. The objectives of this review/clinical technique article are to describe some of the most common clinical situations that occur during endodontic retreatment and to highlight the importance of endodontic retreatment for tooth conservation.
Conclusions: Based on a correct endodontic and restorative diagnosis and continuing with an appropriate endodontic therapy — in this case retreatment — we can maintain a compromised tooth and achieve treatment success, not only through endodontics but also dentistry in general.
Introduction
Endodontic retreatment is defined in the glossary of the American Association of Endodontists (AAE) as the “procedure to remove root canal filling materials from the tooth, followed by cleaning, shaping, and obturating the canals.” This procedure is indicated in teeth where previous endodontic treatment seems inadequate or has failed, or in cases of long-term exposure of root canal filling material to the oral environment leading to apical pathology related to coronal leakage.1
The main cause of initial treatment failure is bacterial persistence within the root canal, or coronal penetration and/or leakage after treatment.2 This would indicate that if the professional can disinfect the root canal system and achieve a tight seal both apically and coronally during retreatment, the success rate would considerably increase. Given the anatomical complexity of the root canal system, the objective of endodontic therapy would be to reduce the bacterial load to levels compatible with host healing.3
Dentists and/or endodontists should be trained to establish a diagnosis from an endodontic and restorative perspective, encompassing not only an endodontic vision of the tooth to be retreated but also a restorative vision. This means that dentists and/or endodontists should evaluate whether retreatment is viable from a pathological point of view and also consider whether the dental element will be structurally suitable for adequate restoration and fully functional in the oral environment after endodontic therapy. As part of this diagnosis process, the tooth needs to be evaluated to rule out any vertical root fracture (VRF) that may be contributing to the endodontic failure that has presented.
Currently, an important tool in endodontics is cone beam computed tomography (CBCT). This technique allows the practitioner to perform a study of the tooth to be retreated in three dimensions (3D), before the actual treatment is initiated, and thus plan the treatment knowing the anatomical and/or iatrogenic obstacles present.4 Additionally, this allows determination of a VRF that often is not evident on traditional radiographs and may be difficult to identify during the clinical exam. A thorough study of the case before the clinical procedure allows the practitioner to determine its prognosis with greater accuracy. Additionally, the ability to detect root fractures or situations that could condition the prognosis is very useful in determining whether to perform the procedure, and especially to be able to explain to the patient the risks and benefits of carrying out the treatment.
The literature reports a success rate ranging from 80% to 88% for endodontic retreatment, thus being a procedure with a predictable prognosis when well performed and, essentially, when there is a correct diagnosis.5 On the other hand, the prognosis will be affected by the type of previous treatment received by the tooth. For example, when there is a perforation or remaining fractured instrument fragment, among other situations, the chances of success will not be the same as if these disadvantages were not present, and the success rate may decrease to 47%.6
Overall, clinical procedures include maneuvers such as crown removal and/or access through the crown; removal of anchoring elements such as pins and posts; and removal of gutta percha, silver cones, pastes, and in some cases, even the removal of fractured instruments from the canals. Once these maneuvers are done, access to the root canal system should be gained for cleaning, shaping, and finally obturating the canal system again.7,8 The operating microscope is noteworthy as an instrument of great importance to address the different clinical complexities and situations mentioned previously, which occur during endodontic retreatment.9
In addition to these aspects, we know that if conditions are favorable, retreatment can be performed in a single operative session.10 Considering that the techniques for adhesive post-endodontic restorations have evolved and been refined in the past few years, we could even permanently seal the access cavity and place the post in the same session if the case warrants it. The main advantages of this procedure would be non-contamination after treatment during restorative procedures and, in turn, the reduction of possible procedural errors due to ignorance of the tooth’s internal anatomy by the dentist who did not perform the endodontic treatment.11
Finally, considering the advances in apical microsurgery and the high success rate — approximately 90% — surgical retreatment should be the treatment option prior to tooth extraction when retreatment cannot be performed by orthograde access, and other clinical factors favor maintenance of the tooth.12
The objectives of this study are to describe some of the most common clinical situations that occur during endodontic retreatment and to highlight the importance of endodontic retreatment for tooth conservation.
Ultrasonic post removal
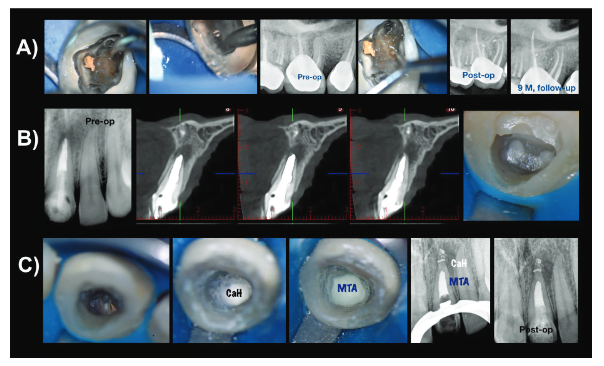
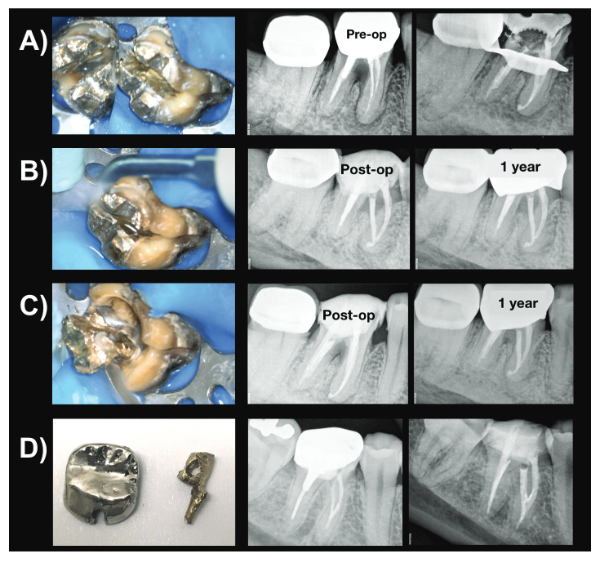
Although there are various mechanical systems for the removal of metallic posts, at present, the tendency is to perform the removal by ultrasonic vibration.8,13 The first thing we should consider in cases of metallic posts is to dislodge them — that is, to eliminate all types of post retention that may exist. Where possible, this should be done at the expense of the metal post and not the tooth remnant. On the other hand, it will depend on the type of post to be removed, regardless of the need to be cut or not. In the case of cast posts on multiradicular teeth anchored to more than one root, it is advisable to cut them with quality metal cutting carbide burs under magnification to avoid damaging the remaining dental tissue during this maneuver (Figure 1A). Cutting is essential for this type of post because root inclination and its multiple anchor points determine that there is no coronal space for the post to pass through if the post is not sectioned. Once the post is sectioned, vibration is performed on the different parts with ultrasonic tips under continuous irrigation until the post is removed (Figures 1B, 1C). Another technique reported in the literature to remove cast posts is to drill the post stump, applying ultrasonic vibration through the hole and thus achieving the removal of the element.14,15 To perform this technique, the posts should be parallel, in case there are more than one or, rather, uniradicular pins. This technique seems to be very effective, greatly reducing the pulling force necessary to remove this type of pin15 (Figure 1D). In the case of metallic prefabricated posts, once their coronal portion is exposed, ultrasonic vibration is performed in a counter-clockwise direction under constant irrigation to facilitate their removal (Figure 2A). Overall, these posts are removed more easily than cast posts. The post removal time would depend on the type of cement used when initially placed and post length, requiring longer times with longer posts.16
Contrary to what has been described about metal posts, in the case of esthetic fiber-reinforced composite posts (FRCPs), commonly known as fiber posts, removal can become more complex. Fiber posts consist of parallel fibers in a resin matrix, and removal is directed to progression to the apical extent of the post down the center of the post working between the fibers. Numerous ultrasonic tips have been designed for this purpose, and removal systems are available, which are usually kits sold for each brand.17,18 These kits are not always available; therefore, a universal technique for all FRCPs is that of wear by ultrasonic vibration under magnification. This technique is also described with diamond burs powered by high-speed handpieces, but currently the use of diamond-coated ultrasonic tips is considered safer. Magnification is important in this procedure to be able to visualize more clearly the edges of the post because the post-cement-dentin interface of FRCPs is very difficult to determine with the naked eye. Once the post is exposed and cut to the level of the canal orifice at the chamber floor, the post is trimmed every 1-2 mm, deepening into the corono-apical direction (Figure 2B) under continuous irrigation until reaching the gutta-percha filling (Figure 2C). Refrigeration by means of irrigation in these procedures is of great importance because ultrasound generates a high temperature, and this is harmful for the dental and supporting tissues.8,13
Removal of root canal filling material
Having removed the anchoring elements, we proceed to the removal of the filling material, which can be gutta percha, endodontic sealant, silver points, pastes, or any combination of these.
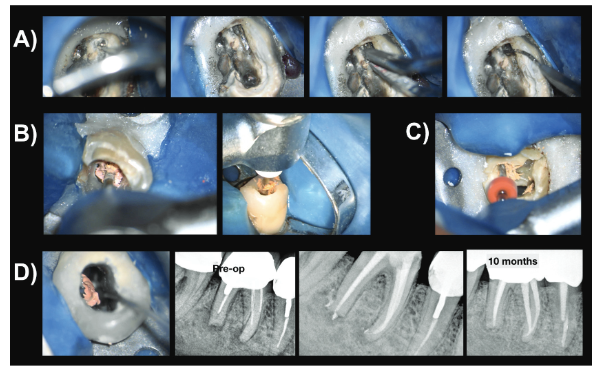
Silver points are root canal filling materials that were used decades ago, still in limited use, but there are currently still cases where they need to be removed. Silver cones are rigid and generally found with some degree of canal mismatch because they are thin, round-shaped, and have a low taper tend to have greater volume of sealer to cone in the canal. Generally, a remnant of these cones is present in the coronal chamber, allowing the practitioner to grasp and remove them with thin tweezers. Additionally, the use of ultrasound to dislodge them, if they are attached to the canal, may be beneficial. This would favor their removal, but on the other hand, they are very fragile. In the presence of excessive ultrasonic vibration or some milling, they may break and become trapped within the canal, complicating their removal. A hand file may be threaded down the side of the silver point, and after penetration several millimeters into the canal, a tug on the file may engage the silver point and dislodge it from the canal. When silver points were used, an amalgam was prepared as a coronal obturation, covered many times by a cast crown. The amalgam should be removed using only rotating burs to break it, then following carefully with ultrasound so as not to make the mistake of cutting the silver cones at the canal opening (Figure 3A).
In general, root canals are usually filled with gutta percha when patients attend the dental clinic. Gutta percha is a thermoplastic material; therefore, there are different techniques for its removal. The traditional technique uses K files or H files, along with chemical solvents such as xylol or chloroform to soften the gutta-percha component of the obturation material, allowing further penetration of the file deeper into the canal. The procedure begins from the crown to the apex, using copious irrigation with a physiological solution and/or sodium hypochlorite along with the removal. Gates burs can be used for the coronal and middle thirds in root canals with very compact fillings. Later, together with mechanized endodontics, different brands of gutta-percha removal systems have emerged. All function in the same way, generally using rotational movement (Figure 3B). Currently, WaveOne® (Dentsply Maillefer, Switzerland) and Reciproc® (VDW, Germany) instruments, of reciprocating motion, have also been suggested to remove gutta percha with very good results reported in the literature19 (Figure 3C). In any case, and considering these varied possibilities, a recommended technique would be to use mechanized systems to remove most root filling material without solvent, and then finish the apical portion or curvatures manually with solvent if necessary.20 Although the use of solvents facilitates the procedure by softening the gutta percha, on the other hand, gutta-percha sticks to the root canal walls, hindering its complete elimination at times.
Residual solvents may hamper contact of the new obturation material (sealer and gutta percha) potentially creating a potential leakage avenue over time. Therefore, its use is recommended only when essential. Currently, the use of ultrasound under magnification is proposed for removing remnants of filling material within the canal and optimizing its cleaning (Figure 3D).
Missed root canals
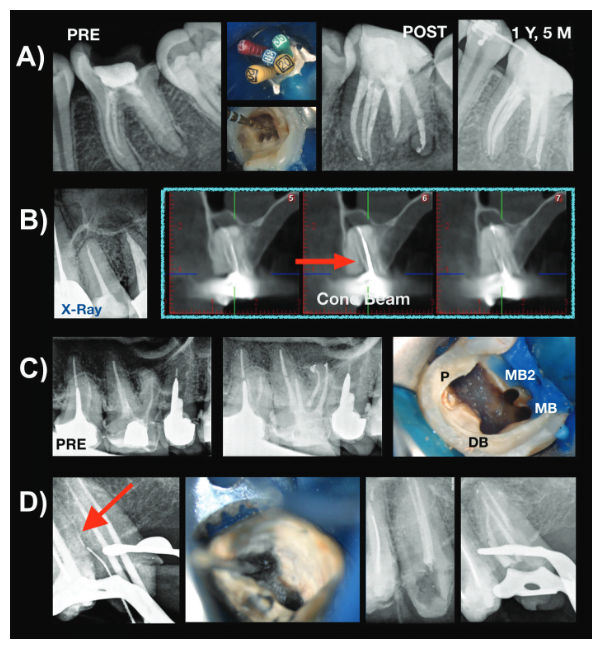
Many times, the cause of initial treatment failure is the presence of bacteria in some missed canals. The most common cases are the second mesiobuccal canal (MB2) of the maxillary first molar, the presence of two canals in the maxillary second premolar, two canals in the lower incisors and premolars, and the presence of two distal canals in the mandibular molars. Rarely, although possible, the presence of the middle mesial canal of the mandibular first molar can be the cause of missed anatomy that leads to the failure of the initial endodontic treatment (Figure 4A). Of all reported cases, the middle mesial canal is the least common.21,22 To determine the presence of these missed canals during diagnosis, when they cannot be clearly visualized in a periapical radiograph, the use of tomography again becomes an important tool in the exploration of these canals and their discovery4,23 (Figure 4B). One of the most common causes of missed canals is MB2. This canal is present in a percentage of cases ranging from 55% to 70% and even up to 80% of cases, according to different authors24,25 Regardless of these numbers, it is striking that the discovery rate of this canal is greater in retreatment than in the initial treatment.26 This could be due to the fact that, in the face of initial treatment failure and while searching for its cause, the dedication of the acting professional to find the root canal is greater (Figure 4C). Another important factor to consider regarding the MB2 canal is that in 39% of cases, it ends in an independent foramen.24 In these cases, the use of tomography can also guide in discovering them and determining their location, to allow planning their search in a predictable manner.4,27
Removal of fractured instruments
In cases of non-surgical retreatment, one of the most complex situations to solve is the removal of fractured instruments from within the canal (Figure 4D). Numerous techniques have been described, from the use of hand files to trap and remove the fragments to countless devices made for this purpose.28 Regarding the use of these specific kits, it is interesting to note that each operator should choose the one considered most appropriate to his/her training.
A universal technique is the use of thin ultrasonic tips under magnification, preferably an operating microscope. The first thing we should achieve is straight access to the instrument to be removed. The technique consists of exposing the instrument from 1 mm to 3 mm in its most coronal portion to be able to perform ultrasonic vibration in that place, thus unlocking the fragment and removing it. The exposed length will also depend on the length of the fragment. This procedure takes time and has to be performed carefully because the space generated to dislodge the fragment is at the expense of dental tissue, structurally weakening the root. This situation can also lead to accidents such as perforations, in the case of not having good vision and fine and precise motion. Therefore, this maneuver should be as conservative as possible.29 Some factors will determine whether to remove the fractured fragment. First, its position in the root canal is essential, considering that the more apical the fragment, the more difficult its removal. Additionally, if the instrument is beyond the curvature of the canal or is not visible, the possibilities decrease from few to none, increasing the risk of complications.30
Treatment of root perforations
Root perforations are mistakes often made during endodontic treatment. Root perforations can occur at different levels, and we could classify them didactically according to their location as occurring in the apical third, middle third, coronal third, or chamber floor. In the apical third, perforations usually occur when there is a ledge, and we try to negotiate the canal; in that attempt, a hole is drilled in the canal, transporting the canal. Perforations can also occur when trying to remove fractured instruments as described previously. In the middle third, the cause is usually due to deviations in post preparation, or in some cases, as in the mesial roots of mandibular molars, it can also be due to excessive wear of the furcal wall during instrumentation-stripping related to the natural concavity on the distal aspect of the mesial root. In the coronal third, perforations usually occur during post preparation or due to errors when accessing the canal in the initial stages of endodontic treatment. The same happens with chamber floor perforations, generally related to a spatial disorientation by the operator when approaching the pulp chamber and searching for the canal opening, which is even greater in cases of very sclerotic pulp chambers due to secondary dentin formation. An important prognostic factor with respect to the perforation site is related to the level of the surrounding bone, whether it is above or below the crestal bone level. Perforation size is also important, being inversely related to the prognosis, and an additional important factor is if the perforation is recent or longstanding.31
Regarding the perforation site, if perforations are above the level of the crestal bone, permanent sealing is more complex, considering that they are practically exposed to the oral environment. In these cases, the materials of choice are usually glass ionomers or composite resins. On the other hand, in cases of perforations below the crestal bone or chamber floor levels, the material of choice is mineral trioxide aggregate (MTA), with many years of studies on this matter.32-34 The use of new bioceramics materials is also currently suggested.35 In the case of chamber floor perforations, which are usually the most common, it is important to consider at the time of diagnosis whether they are recent or longstanding. The difference if they are longstanding is that they usually have an associated osseous lesion. Treatment in these cases begins with curettage of the granulation tissue occupying the space of the osseous lesion with excavators or ideally with electrocautery/lasers. The edges of the perforation are then cleaned with ultrasound because they are probably contaminated. And finally, in these cases, before placing MTA into the perforation site, it is optional to place a collagen membrane or similar in the space of the lesion, as is the use of calcium hydroxide, in order to generate a barrier preventing extrusion of the MTA repair material.36 Use of the barrier membrane limits excess repair material from extruding into the space left by the osseous lesion and allow osseous healing with bone fill over time.
Discussion
Endodontic retreatment, in either an orthograde or retrograde direction according to the case, should be the option of choice before tooth extraction and implant placement when the tooth is structurally sound and periodontal conditions warrant maintenance of the tooth. Numerous procedures described in this study were analyzed in order to perform endodontic retreatment. Dental implants are the ideal alternative to replace a tooth that cannot be treated, and they have a good prognosis. It is for this reason that, before making the decision to perform tooth extraction, the dentist/endodontist should perform a multidisciplinary evaluation.37
The use of technology in endodontic retreatment, such as the use of CBCT for diagnosis and magnification in dental clinical practice, allows us to perform procedures that are more predictable. The clinical procedure of endodontic retreatment under the operating microscope allows us to deal with highly complex cases and improve the scope of our treatment and its prognosis, always with the help of adequate operator training.9,38 In addition, ultrasound becomes an instrument of great utility in most stages of endodontic therapy, especially nonsurgical and surgical retreatment.13
Once the tasks of removing anchors and obturation materials, sealing of perforations, etc., are completed, shaping and disinfection of the root canal are essential to be able to re-seal it properly. Depending on the clinical criteria of the operator, the placement of a new post or final restoration is recommended to avoid contamination of the retreated root canals.10 An adequate coronal seal is essential to prevent coronal leakage and achieve the success of our therapies — that is, the health of the periradicular periodontium.39,40 Although the coronal seal improves the prognosis of retreatment, other factors affecting it could be the size of the previous peri-radicular lesion, the presence of perforations, or the impossibility of achieving an apical seal, among others.41 According to a review by Ng, et al., the 4-year survival rate was similar between initial treatment and retreatment, reaching 95%.42
Tooth maintenance implies preserving the periodontium, which results in preserving bone and gingival levels, which have a great esthetic value in dentistry these days. Many times, tooth extraction may be a simpler alternative than endodontic retreatment, but that should not be the reason for the decision.43 In regard to making a referral or making the decision to maintain or replace a dental element, it is very important that general dentists know the possibilities of current endodontic treatment and its benefits.44,45
The success of a dental implant or an endodontic treatment depends in turn on the experience of the operator; this means that statistics and published review studies in both specialties may not always reveal the current reality of the specialty. It is for this reason that publications in this regard should be carefully read and understood so as not to be influenced by results that may not be appropriate. Both therapies, correctly chosen and carried out, are intended to return the patient’s health along with masticatory function and esthetics. It is inadequate to analyze them as competing procedures — endodontics versus implant; they should be considered complementary procedures to restore the patent’s oral health.43
Conclusions
Based on a correct endodontic and restorative diagnosis and continuing with appropriate endodontic therapy — in this case retreatment — we can maintain a compromised tooth and achieve treatment success, not only through endodontics but also dentistry in general. An adequate coronal restoration and routine follow-ups are essential to evaluate the long-term success of our therapies.
Acknowledgment: Dr. Alberdi extends his appreciation to Dr. Fernando Goldberg for his guidance in the writing of this manuscript.
Dr. Peter Raftery discussed his ideas about correct endodontic and restorative diagnosis and minimally invasive techniques. Check out his article here.
- American Association of Endodontists. Glossary of Endodontic Terms. 2016. https://www.aae.org/clinical-resources/aae-glossary-of-endodontic-terms.aspx. Accessed November 19, 2018.
- Ricucci D, Siqueira JF Jr, Bate AL, Pitt Ford TR. Histologic investigation of root canal-treated teeth with apical periodontitis. A retrospective study from twenty-four patients. J Endod. 2009;35(4):493-502.
- Siqueira JF Jr, Roças IN. Clinical implications and microbiology of bacterial persistence after treatment procedures. J Endod. 2008,34(11):1291-1301.
- AAE and AAOMR Joint Position Statement: Use of Cone Beam Computed Tomography in Endodontics 2015 Update. J Endod. 2015;41(9):1393-1396.
- Imura N, Pinheiro ET, Gomes BP, et al. The outcome of endodontic treatment: a retrospective study of 2000 cases performed by a specialist. J Endod. 2007;33:1278-1282.
- Gorni FG, Gagliani MM. The outcome of endodontic retreatment: a 2-yr follow-up. J Endod. 2004;30(1):1-4.
- Goldberg F, Cantarini C. El retratamiento endodóntico: consideraciones clínicas. Rev Asoc Odontol Argent. 2014; 102(2):76-82.
- Ruddle CJ. Nonsurgical Retreatment. J Endod. 2004;30(12): 827-845.
- AAE Special Committee to Develop a Microscope Position Paper. AAE Position Statement. Use of microscopes and other magnification techniques. J Endod. 2012;38(8):1153-1155.
- Moreira MS, Anuar ASN, Tedesco TK, Dos Santos M, Morimoto S. Endodontic treatment in single and multiple visits: an overview of systematic reviews. J Endod. 2017;43(6):864-870.
- Schwartz RS, Fransman R. Adhesive dentistry and endodontics: materials, clinical strategies and procedures for restoration of access cavities: a review. J Endod. 2005;31(3):151-165.
- Kim S, Kratchman S. Modern endodontic surgery concepts and practice: a review. J Endod. 2006;32(7):601-623.
- Plotino G, Pameijer CH, Grande N, Somma F. Ultrasonics in endodontics: a review of the literature. J Endod. 2007;33(2):81-95.
- Zuolo ML, Kherlakian D, de Mello JE Jr, de Carvalho MCC, Fagundes MIRC. Reintervención en Endodoncia. Sao Paulo, Brazil: Santos Editora; 2012.
- Graça IAA, Sponchiado Júnior EC, Marques AAF, de Moura Martins L, Garrido ÂDB. Assessment of a cavity to optimize ultrasonic efficiency to remove intraradicular posts. J Endod. 2017;43(8):1350-1353.
- Ebrahimi Dastgurdi M, Khabiri M, Khademi A, Zare Jahromi M, Hosseini Dastnaei P. Effect of post length and type of luting agent on the dislodging time of metallic prefabricated posts by using ultrasonic vibration. J Endod. 2013;39(11):1423-1427.
- Scotti N, Bergantin E, Alovisi M, Pasqualini D, Berutti E. Evaluation of a simplified fiber post removal system. J Endod. 2013;39(11):1431-1434.
- Lindemann M, Yaman P, Dennison JB, Herrero AA. Comparison of the efficiency and effectiveness of various techniques for removal of fiber posts. J Endod. 2005;31(7):520-522.
- Colaco AS, Pai VAR. Comparative Evaluation of the Efficiency of Manual and Rotary Gutta-percha Removal Techniques. J Endod. 2015; 41:1871–1874.
- Colaco AS, Pai VAR. Comparative evaluation of the efficiency of manual and rotary gutta-percha removal techniques. J Endod. 2015;41(11):1871-1874.
- Nosrat A, Deschenes RJ, Tordik PA, Hicks ML, Fouad AF. Middle mesial canals in mandibular molars: incidence and related factors. J Endod. 2015;41(1):28-32.
- Tahmasbi M, Jalali P, Nair MK, Barghan S, Nair UP. Prevalence of middle mesial canals and isthmi in the mesial root of mandibular molars: an in vivo cone-beam computed tomographic study. J Endod. 2017; 43(7):1080-1083.
- Michetti J, Maret D, Mallet JF, Diemer F. Validation of cone beam computed tomography as a tool to explore root canal anatomy. J Endod. 2010;36(7):1187-1190.
- Briseño-Marroquín B, Paqué F, Maier K, Willershausen B, Wolf TG. Canal morphology and configuration of 179 maxillary first molars by means of micro-computed tomography: an ex vivo study. J Endod. 2015;41(12):2008-2013.
- Wolcott J, Ishley D, Kennedy W, Johnson S, Minnich S. Clinical investigation of second mesiobuccal canals in endodontically treated and retreated maxillary molars. J Endod. 2002;28(6):477-479.
- Wolcott J, Ishley D, Kennedy W, et al. A 5 yr clinical investigation of second mesiobuccal canals in endodontically treated and retreated maxillary molars. J Endod. 2005; 31(4):262-264.
- Hiebert BM, Abramovitch K, Rice D, Torabinejad M. Prevalence of second mesiobuccal canals in maxillary first molars detected using cone-beam computed tomography, direct occlusal access, and coronal plane grinding. J Endod. 2017;43(10):1711-1715
- Terauchi Y, O’Leary L, Kikuchi I, et al. Evaluation of the efficiency of a new file removal system in comparison with two conventional systems. J Endod. 2007;33(5):585-588.
- Terauchi Y, O’Leary L, Suda H. Removal of separated files from root canals with a new file-removal system: case reports. J Endod. 2006;32(8):789-797.
- Souter NJ, Messer HH. Complications associated with fractured file removal using an ultrasonic technique. J Endod. 2005;31(6):450-452.
- Tsesis I, Rosenberg E, Faivishevsky V, et al. Prevalence and associated periodontal status of teeth with root perforation: a retrospective study of 2,002 patients’ medical records. J Endod. 2010;36(5):797-800.
- Pontius V, Pontius O, Braun A, Frankenberger R, Roggendorf MJ. Retrospective evaluation of perforation repairs in 6 private practices. J Endod. 2013;39(11):1346-1358.
- Torabinejad M, Chivian N. Clinical applications of mineral trioxide aggregate. J Endod. 1999;25(3):197-205.
- Parirokh M, Torabinejad M. Mineral trioxide aggregate: a comprehensive literature review—Part I: chemical, physical, and antibacterial properties. J Endod. 2010;36(1):16-27.
- Torabinejad M, Parirokh M, Dummer PMH. Mineral trioxide aggregate and other bioactive endodontic cements: an updated overview—Part II: other clinical applications and complications. Int Endod J. 2018;51(3):284-317.
- Pace R, Giuliani V, Pagavino G. Mineral trioxide aggregate as repair material for furcal perforation: case series. J Endod. 2008;34(9):1130-1133.
- Iqbal MK, Kim S. A review of factors influencing treatment planning decisions of single-tooth implants versus preserving natural teeth with nonsurgical endodontic therapy. J Endod. 2008;34(5):519-529.
- Khalighinejad N, Aminoshariae A, Kulild JC, et al. Effect of the dental operating microscope on the outcome of nonsurgical root canal treatment: a retrospective case-control study. J Endod. 2017;43(5):728-732.
- Gomes AC, Nejaim Y, Silva AIV, et al. Influence of endodontic treatment and coronal restoration on status of periapical tissues: a cone-beam computed tomographic study. J Endod. 2015;41(10):1614-1618.
- Craveiro MA, Fontana CE, de Martin SA, Bueno CE. Influence of coronal restoration and root canal filling quality on periapical status: clinical and radiographic evaluation. J Endod. 2015;41(6)836-840.
- Ng YL, Mann V, Gulabivala K. A prospective study of the factors affecting outcomes of nonsurgical root canal treatment: part 1: periapical health. Int Endo J. 2011;44(7):583-609.
- Ng YL, Mann V, Gulabivala K. A prospective study of the factors affecting outcomes of nonsurgical root canal treatment: part 2: tooth survival. Int Endod J. 2011;44:610-625.
- Setzer FC, Kim S. Comparison of long-term survival of implants and endodontically treated teeth. J Dent Res. 2014;93(1):19-26.
- Hannahan JP, Eleazer PD. Comparison of success of implants versus endodontically treated teeth. J Endod. 2008;34(11):1302-1305.
- Doyle SL, Hodges JS, Pesun IJ, Baisden MK, Bowles WR. Factors affecting outcomes for single-tooth implants and endodontic restorations. J Endod. 2007;33(4):399-402.
Stay Relevant With Endodontic Practice US
Join our email list for CE courses and webinars, articles and more..
