Dr. Allen Ali Nasseh offers a review of an integral part of endodontic therapy
Exactly 10 years ago, the first, and still the only premixed nano-particulate bio-ceramic cement was FDA approved for use as a universal root canal cement. The first two formulations were the Endosequence® BC Sealer™ and Endosequence® RRM™ (Brasseler USA, Savannah, Georgia) and were soon followed by a thicker, faster setting putty-like formulation called BC Putty FS (Brasseler USA, Savannah, Georgia).

Figure 1: A premolar and molar teeth in the maxillary left quadrant (teeth Nos. 12 and 14) were treated nonsurgically with hydraulic condensation in 2008 and subsequently recalled for evaluation in 2016. The patient was nonsymptomatic, and both teeth had healed lesions. Most importantly, the original sealer puffs were present, and the sealer showed perpetual integrity over the 8-year period
The very first bioceramic material in endodontics dates back to 1993; it was mineral trioxide aggregate (MTA) which was introduced for surgical root repair. MTA’s exceptional histological response was the impetus behind the development of the nano-particulate premixed bioceramics for nonsurgical use. These newer bioceramics were designed from the ground up with the intent of taking full advantage of MTA’s biocompatibility, bonding capability, dimensional stability, non-resorbability, and hydrophilic qualities without some of its unnecessary components such as calcium aluminate and bismuth oxide impurities, which caused potential toxicity and dentin staining during endodontic clinical use.1-3
Therefore, a smaller particle size formulation was designed de novo, using a patented premix delivery method to allow improved delivery of bioceramics and expand its use from surgical repair materials into the realm of nonsurgical root canal therapy as an obturation cement and a filler.
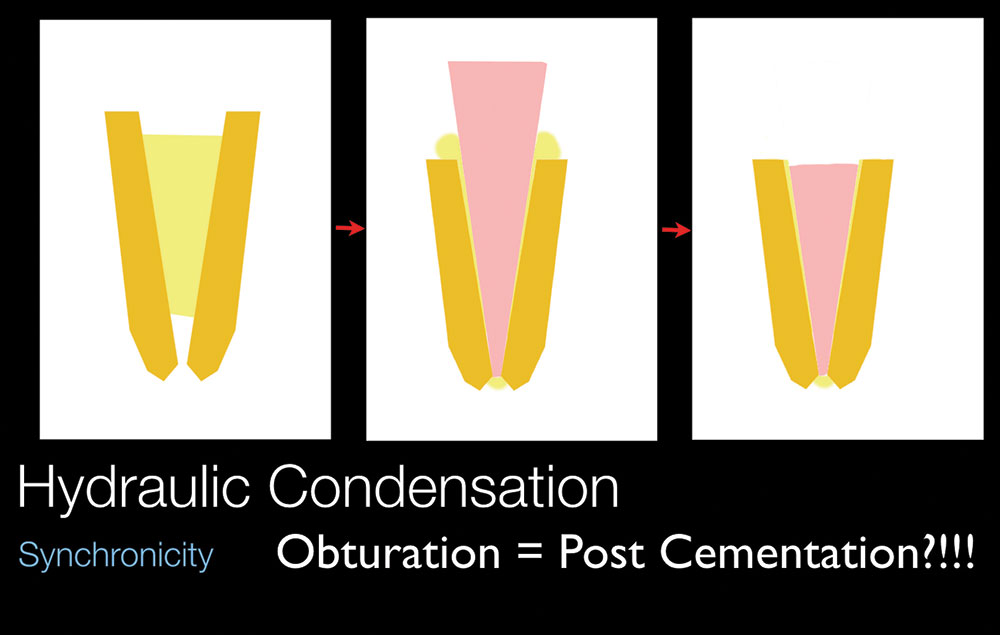
Figure 2: Hydraulic Condensation consists of placing the bioceramic cement in the canal and then seating a pre-fitted bioceramic coated GP cone all the way to full length. The cone is then seared off at the orifice and condensed apically. Since the cone is a slightly higher melting point, it acts as a plugger pushing the BC filler in the canal. This is similar to the concept of post cementation except that the cone reaches the apex and provides a path for retreatment if necessary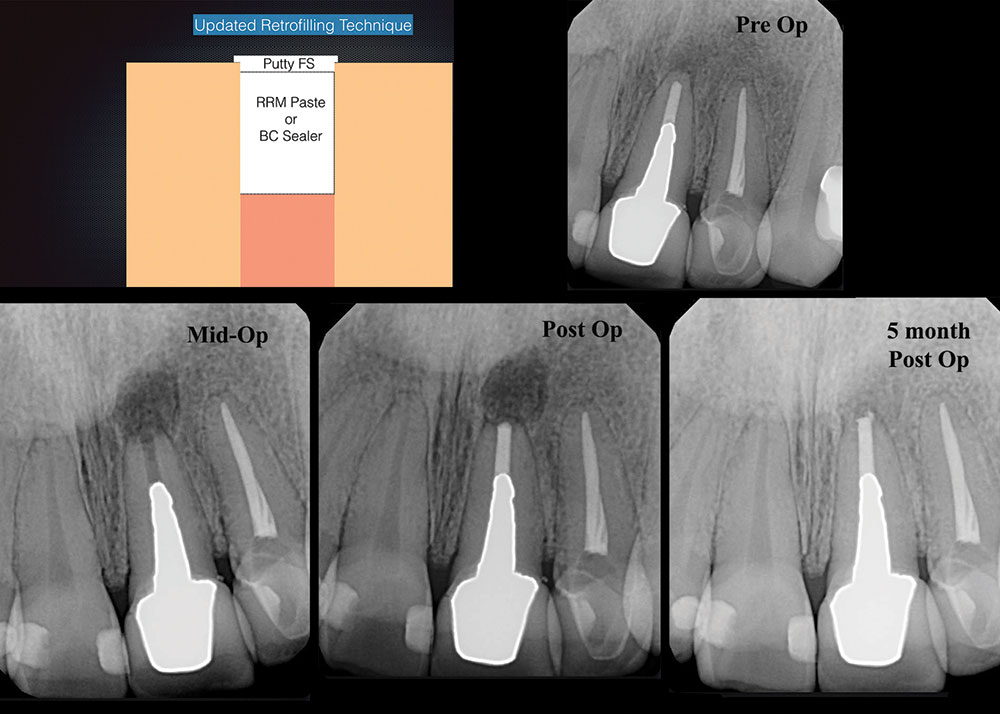
Figure 3: A retrofilling technique called the “Lid Technique” was developed by RWE to make the most of combining the light body effects of RRM syringeable material (injection into the retropreparation) followed by placing a lid of the BC Putty to protect this material during the setting period. This technique helps make the retrofilling process very efficient
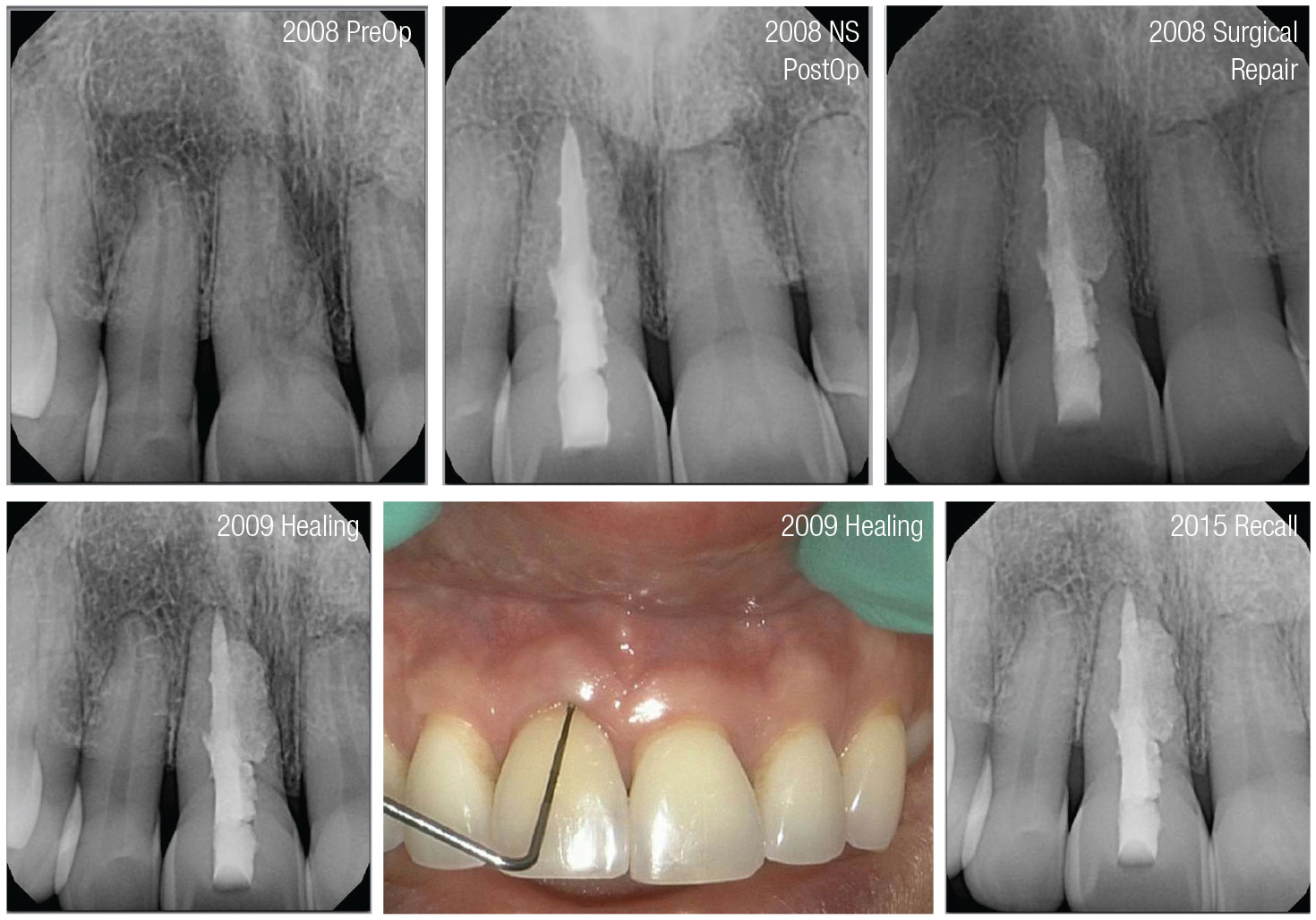
Figure 4: A large external resorptive defect in tooth No. 8 is treated nonsurgically with RRM Sealer and then flapped back for direct surgical repair using RRM Putty. One year and 7-year followups show great healing of the tissue and bone
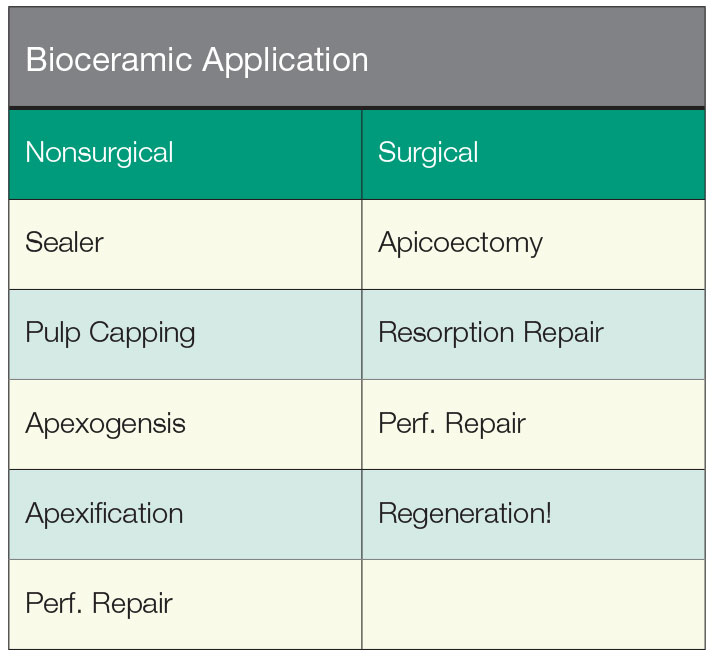
Figure 5: Nonsurgical and surgical application of bioceramic cements
Figure 6: The three main formulations of the nanoparticulate bioceramics (The Sealer, RRM, and Putty FS) can be used together or alone in many different applications of endodontic care both nonsurgically as well as surgically
Real World Endo® (Boston, Massachusetts) developed techniques for the use of these materials prior to their FDA approval and designed nonsurgical and surgical techniques called the Hydraulic Condensation Technique and the Lid Technique to harness the power of bioceramic technology to improve efficiency of nonsurgical and surgical obturation while still allowing this material to be retreatable if needed.4-6 The dimensional stability, bonding, and non-resorbability of these materials allowed these techniques to be developed. Figure 1 shows a nonsurgical root canal therapy in a maxillary premolar and molar under a bridge performed in 2008 and recalled in 2016. The radiographs show the stability of the cement over the 8-year period (Figure 1). The non-solubility and dimensional stability of the cement allows cementation of a bioceramic-coated master cone that is matched with the Master File to be seated to full length using the bioceramic cement as the interface to fill in any gaps. The gutta-percha cone in this technique acts as both a cement delivery tool and filler while providing a predictable path for retreatment if needed. The actual seal is provided by the chemically bonding bioceramic cement, and the technique resembles the cementation of a passive post (Figure 2).
Real World Endo® later designed the BC Putty specifically for surgical use, which allowed efficient repair with this bioceramic formulation without the handling limitations and staining side effects related to the bismuth oxide present in conventional MTA. The surgical use of the putty ranges from surgical apicoectomy and retrofilling (Figure 2), external root resorption or perforation repair (Figure 3), and many other uses such as pulpotomy, pulp capping, and regenerative procedures (Figure 5). Since the composition and material properties of the bioceramic line are the same as MTA, the same surgical and nonsurgical applications of MTA apply to these materials plus the ability to use them as a root canal cement due to the much smaller particle size. The improved clinical handling properties due to their premix nature and no dentin staining due to the absence of bismuth oxide are the main advantages of these products over MTA. BC Sealer, RRM, and Putty are three different viscosities of the same base premixed calcium silicate, calcium phosphate bioceramic that have been used for a decade and after being on the market for 10 years, and after millions of surgical and nonsurgical clinical cases, they’re time tested and growing rapidly in popularity (Figure 5).
In conclusion, bioceramic materials are now an integral part of endodontic therapy, and the three premixed nano particulate bioceramic formulations discussed provide excellent clinical handling that can be used for the same clinical applications as MTA with the addition of nonsurgical root canal obturation. After 10 years of clinical experience and availability, the use of these materials is well accepted by the endodontic community, and these materials are now ready for prime time.
 Allen Ali Nasseh, DDS, MMSc, received his dental degree from Northwestern University Dental School in Chicago, Illinois, in 1994 and completed his postdoctoral endodontic training at Harvard School of Dental Medicine in 1997, where he also received a Masters in Medical Sciences (MMSc) degree in the area of bone physiology. He has been a clinical instructor and lecturer in the postdoctoral endodontic program at Harvard School of Dental Medicine since 1997 and the Alumni Editor of Harvard Dental Bulletin. Dr. Nasseh is the endodontic advisor to several educational groups and study clubs and is endodontic editor to several peer-reviewed journals and periodicals. He has published numerous articles and lectures extensively nationally and internationally in surgical and nonsurgical endodontic topics. Dr. Nasseh is in solo private practice (MSEndo.com) in downtown Boston, Massachusetts.
Allen Ali Nasseh, DDS, MMSc, received his dental degree from Northwestern University Dental School in Chicago, Illinois, in 1994 and completed his postdoctoral endodontic training at Harvard School of Dental Medicine in 1997, where he also received a Masters in Medical Sciences (MMSc) degree in the area of bone physiology. He has been a clinical instructor and lecturer in the postdoctoral endodontic program at Harvard School of Dental Medicine since 1997 and the Alumni Editor of Harvard Dental Bulletin. Dr. Nasseh is the endodontic advisor to several educational groups and study clubs and is endodontic editor to several peer-reviewed journals and periodicals. He has published numerous articles and lectures extensively nationally and internationally in surgical and nonsurgical endodontic topics. Dr. Nasseh is in solo private practice (MSEndo.com) in downtown Boston, Massachusetts.
Disclosure: Dr. Nasseh is the President and Chief Executive Officer for the endodontic education company Real World Endo® (RealWorldEndo.com).
- Zhang W, Li Z, Peng B. Ex vivo cytotoxicity of a new calcium silicate-based canal filling material. Int Endod J. 2010;43(9):769-774.
- Ma J, Shen Y, Stojicic S, Haapasalo M. Biocompatibility of two novel root repair materials. J Endod. 2011;37(6): 793-798.
- Keskin C, Demiryurek EO, Ozyurek T. Color stabilities of calcium silicate-based materials in contact with different irrigation solutions. J Endod. 2015;41(3):409-411.
- Nasseh AA. The rise of bioceramics. Endodontic Practice US. 2009;2:17-22.
- Koch K, Brave GD, Nasseh AA. Bioceramic technology: closing the endo-restorative circle, part 1. Dent Today. 2010;29(2):100-105
- Koch K, Brave GD, Nasseh AA. Bioceramic technology: closing the endo-restorative circle, part 2. Dent Today. 2010;29(3):98, 100, 102-105.
Stay Relevant With Endodontic Practice US
Join our email list for CE courses and webinars, articles and more..
