CE Expiration Date: September 1, 2026
CEU (Continuing Education Unit):2 Credit(s)
AGD Code: 070
Educational aims and objectives
This self-instructional course for dentists aims to explore concepts and innovations in endodontic irrigation, with specific focus on the use of uncomplicated and affordable sonic/ultrasonic devices to activate or agitate solutions during the cleaning phase, while using more efficient combined disinfecting solutions during the disinfection phase of irrigation.
Expected outcomes
Endodontic Practice US subscribers can answer the CE questions by taking the quiz online at endopracticeus.com to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can:
- Define the overall goals of irrigation.
- Define Macro Debris Removal (MDR) and its role in the process.
- Identify the importance of agitation and activation techniques in the cleaning process.
- Recognize the main requirements for adequate
- List the three steps to highly expedite the cleaning and disinfection components of irrigation.
- Identify the three main chemical needs of all endodontic irrigation.
Dr. Allen Ali Nasseh writes about effective cleaning and disinfection of the root canal space, and possible challenges and solutions. Find out about how to reach the goals of irrigation, and subscribers can get 2 credits by taking our CE quiz!
Allen Ali Nasseh, DDS, MMSc, outlines innovations and concepts for effective cleaning and disinfection
Endodontic irrigation plays a pivotal role in the success of clinical endodontics.1,2 Traditionally, the term “irrigation” has been used broadly to explain disinfection of root canal spaces. However, recent advancements in powered devices and chemical solutions have led the author to conclude that the term irrigation is better understood if broken down into its two distinct subcategories: cleaning and disinfection.3 This conceptual breakdown helps the clinician focus on the specific needs of each component of irrigation, focusing on optimizing its requirements for better efficiency. The overall goals of irrigation can be described as the chemical and physical removal of organic and inorganic debris followed by disinfection and removal of microbes and microbial components from the root canal space.1,4
During the cleaning component of irrigation, techniques, and processes aim at the physical removal of the macro debris generated during the act of instrumentation, referred to by the author as Macro Debris Removal (MDR), while disinfection primarily focuses on chemical and physical means to eliminate microorganisms in the root canal space3 (Figure 1).

The Macro Debris Removal (MDR) steps are those cleaning steps that remove the vital or diseased pulpal tissue, dentinal chips, and other debris produced by shaping instruments, as well as the naturally existing loose organic and inorganic debris in the root canal system. These types of macro debris have traditionally been removed by positive pressure syringe irrigation using various irrigation solutions.1
Disinfection, on the other hand, attempts to chemically destroy the biofilm and microorganisms in the root canal system during or after MDR has been accomplished. This article aims to explore concepts and innovations in endodontic irrigation, with specific focus on the use of uncomplicated and affordable sonic/ultrasonic devices to activate or agitate solutions during the cleaning phase, while using more efficient combined disinfecting solutions during the disinfection phase of irrigation.
Cleaning: the importance of agitation and activation techniques
Cleaning the root canal space prior to engaging in disinfection is crucial because clumped macro debris and smear layer in the canal can prevent disinfectant solutions from reaching or contacting the biofilm and microorganism in fins and fissures of the root canal space and can act as a protective barrier for the microorganisms in the canal.5 This smear layer can clog dentinal tubules and physically prevent disinfectants from penetrating into them. Furthermore, we know that our gold standard disinfectant, sodium hypochlorite, is chemically deactivated and buffered rapidly by loose dentinal chips and dentinal walls and loses its efficacy6; therefore, removal of the loose macro debris and dentinal chips will not only expedite shaping, but more importantly, it will help improve the efficacy of the disinfection phase.
Root canal instrumentation produces loose chunks of dentin during the enlargement and advancement of rotary or reciprocating files in the root canal. Although some instrumentation motions generate more debris than others, all instrumentation motions, including reciprocation, rotation, and filing create debris that must be managed promptly to improve disinfection.
Persistent debris in the root canal during instrumentation will cause packing of debris laterally and apically, causing a variety of undesirable mid-operative and postoperative problems including canal blockage, ledging, and post-op pain. Furthermore, packed debris into a file’s dentinal chips will prevent file advancement and can cause file fractures by over-torqueing the instrument. This is why debris management is crucial during all phases of instrumentation.
Historically, most clinicians have used alternating use of sodium hypochlorite, a disinfectant capable of organic tissue dissolution, with a chelating agent like EDTA that removes inorganic components of the dentinal smear layer. This combination has constituted the positive pressure syringe irrigation that has been the standard irrigation for the past century. However, the use of a caustic irrigant such as NaClO in positive pressure to flush out debris bears its own risks. NaClO solution extrusion from the apex can lead to acute postoperative pain, or worse, a hypochlorite accident. This fear has prevented users from imposing a strong flushing action on the syringe solution to avoid these potential procedural accidents, thus resorting to passive needle irrigation to reduce risk. This physically gentler form of irrigation is not as efficient in flushing out loose debris from the canal. This is why the author believes continuous irrigation and activation of gentler solutions, such as distilled or iodinated water, from an ultrasonic or sonic device connected to the fluid source throughout instrumentation, is not only a more efficient method of MDR; but also, it’s a safer method of positive pressure flushing since the activated solution is water and not a toxic chemical.
This process of continuous water flushing using a powered device during instrumentation is often referred to as continuous ultrasonic irrigation.7 The technique involves short interval ultrasonic/sonic use with a wet tip (an ultrasonic or sonic tip with a water port) at a low power setting in each canal in between instrumentation. This can be a 10-15 second burst of water flushing by activating the ultrasonic tip inside the canal and moving up and down. The expressed water from the powered device’s tip will quickly flush the canal from loose macro debris. Since this powered action of water can be used either through ultrasonic or sonic power, the author refers to this technique as “powered flushing” — the act of flushing out the loose content of the canal with a powered ultrasonic or sonically energized continuous flow of water used in a short burst.
However, since water is chemically inert in the canal, once the flushing action is complete, it should be replaced with a chemically active disinfectant. This can be accomplished efficiently with the insertion of a thin negative-pressure suction tip in the canal (Figure 2), creating negative pressure to suction out the water.3 A side benefit of using negative pressure (suction) at this stage to remove the water is the simultaneous removal of any remaining loose debris in the canal suspended in the water or loose that was not removed by powered flushing.

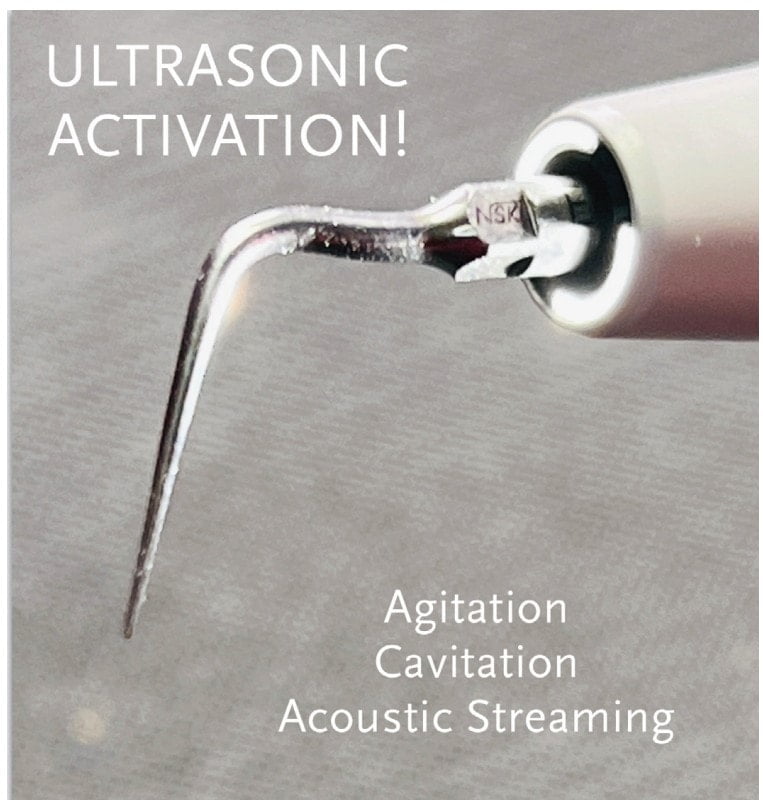
Why are activation and agitation methods important during root canal cleaning procedures? These physical processes are essential because they increase the kinetic energy of the solutions used, which catalyzes the chemical effect of irrigants and enhances the physical removal of debris from the walls of the root canal.7,8 The use of activation or agitation methods, such as ultrasonics or sonic devices, creates an energy wave that propagates throughout the solution, aiding in the removal of loose debris. In case of ultrasonics, this can include cavitation, agitation, and acoustic streaming, all of which increase the kinetic energy of water molecules and their Brownian motion. This continuous flushing of water also facilitates cleaning by creating a streaming effect that washes out the loosened debris from the root canal. To achieve this, connecting an ultrasonic or sonic handpiece to the dental unit with a wet tip that can support continuous water flow during use is recommended.
The overall goals of irrigation can be described as the chemical and physical removal of organic and inorganic debris followed by disinfection and removal of microbes and microbial components from the root canal space.”
The only limitation with the use of ultrasonic tips in this step is the stiffness of ultrasonic tips and the curve of some root canals. Stiff tips cannot negotiate around curves, and this limits their penetration to the straight portion of the root canal. However, even though true ultrasonic activation through cavitation may not occur far beyond the tip of the instrument, agitation and acoustic streaming can still occur several millimeters beyond the instrument tip, thus still improving the kinetic energy of the solution beyond the tip of the instrument and still providing an environment that is superior to mere passive action of the fluids at the apex to flush loose debris.
Therefore, during the cleaning phase of irrigation, which is generally during instrumentation and between files, MDR is safely and efficiently implemented when an ultrasonic or sonically powered wet tip produces continuous flow of energized water to flush out the cut debris from the root canal with positive pressure agitation. This is referred to by the author as “powered flushing.” The remaining water in the root canal is then quickly removed using a negative pressure tip (suctioned out) and is immediately replaced with a disinfectant.
Disinfection: the main requirements for adequate disinfection
After effective MDR has been achieved using powered flushing, the remaining water in the canal is removed with negative pressure suction and replaced with a chemically active solution to achieve deep disinfection.
The requirement for adequate disinfection of the root canal can be summarized as the physical and chemical removal of loose and attached biofilms, as well as their antigenic organic byproducts (e.g., LPS, EPS, etc.). MDR is responsible for the physical removal of the macro debris and physical flushing of some of the biofilm and its associated bacteria, but disinfection is the next level of chemical warfare needed to eradicate the remaining microorganisms and biofilms; and therefore, requires solutions that are optimized for that purpose.
To achieve such chemistry, we need to pay attention to the three main chemical needs of all endodontic irrigation: the removal of the organic debris, the inorganic debris, and the remaining microorganisms and their byproducts.
Over the past 3 decades, we’ve come to consensus that sodium hypochlorite (NaClO) is the gold standard for endodonic disinfection.9 This is due to the fact that higher concentrations (above 2.5%) of NaClO can kill microorganisms as well as dissolve collagen found in tissues. This organic tissue dissolution and simultaneous disinfection has made NaClO an excellent double action irrigant.9 However, since it’s unable to do any inorganic debris removal, the third requirement of irrigation has been assigned to a separate irrigant that is an acid chelator. Recently, the use of EDTA 17% has become popular; however, EDTA and NaClO have a chemically antagonistic relationship and neutralize and buffer each other readily when combined.
Furthermore, NaClO is also buffered by dentinal chips. This means that the use of a chelator to remove dentinal chips is necessary in order to improve the disinfecting function of NaClO. This antagonistic relationship between these two solutions has led clinicians to develop complicated protocol-and-use-separate NaClO and EDTA syringes alternating their use during instrumentation to achieve chelation of dentinal chips followed by disinfection and tissue dissolution.
Since this is a redundant and cumbersome protocol, combining solutions that can achieve these three main objectives of irrigation chemicals has been a long goal in the field. Recently, a new combined irrigation solution has been developed that is a combined 4% NaClO and 11 gentle chelators that substitute EDTA, chemical surfactants, and saponification agents. The replacement of EDTA with other chelators instead of replacing NaClO as a disinfectant allowed the use of the gold standard disinfectant in our field and simultaneous chelation using other chelating agents that are more resistant to the corrosive effect of NaClO. A mix-to-use delivery method was designed to mix the chelators and NaClO before use, allowing ample time for any given procedure using a single irrigation syringe that contains all the necessary components of disinfection and smear layer removal with added surfactants.10
The antimicrobial properties of the new solution, Triton® (Brasseler USA, Savannah, Georgia) have shown it to be 210 times more effective at killing C. albicans compared to NaClO with EDTA.11 Additionally, another study at University of British Columbia has shown that Triton can cut irrigation time by up to 50% thus allowing for a more efficient disinfection routine.12
This combined irrigant has made it possible to achieve simultaneous chelation during disinfection, which was long promised to expedite disinfection and be more efficacious in its action.11,12 Furthermore, adding surfactants to this solution can help deeper penetration into dentinal tubules.11 Recent studies on this combined disinfectant are very promising.13 Given its chemical and ergonomic advantages, this makes this mixture an ideal replacement solution for water immediately after powered flushing of the root canal space during the cleaning phase of irrigation.
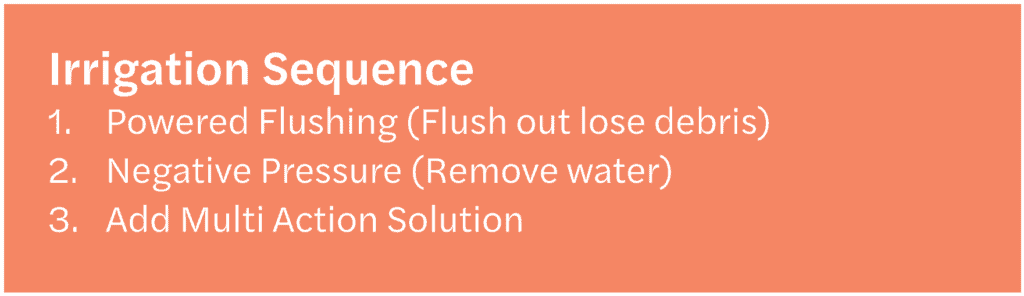
Therefore, removing the macro debris using powered flushing followed by replacing the water in the canal with a combined irrigation solution can help create a more efficient and thorough cleaning and disinfection process. The following three steps highly expedite the cleaning and disinfection components of irrigation:
- Powered flushing
- Negative pressure to remove water
- Replacement with a multi-action irrigant (Figure 4).
Since we know that utilizing passive, positive pressure irrigation, 40 minutes of exposure to NaClO is necessary to kill e. faecalis, it’s possible that a protocol that allows powered flushing with a more efficient irrigation solution can help us overcome this rate-limiting step of disinfection during our root canal procedures by catalyzing the rate of reactions inside the root canal.14 Further research in this area is necessary to validate this claim.
The additional use of Passive Ultrasonic Irrigation (PUI) at the end of the cleaning and shaping procedure, by applying sonic or ultrasonic energy without water in a canal flooded with this combined solution and agitating for an additional 30-60 seconds may achieve an even deeper smear layer removal and disinfection prior to drying and filling the root canal.
Conclusion
In conclusion, it is vital to break down the term irrigation into its two primary components: cleaning and disinfection. The first step, cleaning, involves the removal of macro debris through the use of agitation or activation by a powered device using a safe irrigant like water. The second step entails using negative pressure, specifically micro-suction, to evacuate the water and any loose debris from the root canal. Finally, in the third step, a combined chelator and disinfectant is introduced to fill the canal and allow for continuous chelation during instrumentation. With the availability of simple and cost-effective technology, these three steps can be seamlessly executed, ensuring safe and efficient irrigation during chemomechanical instrumentation.
Find out what has inspired Dr. Nasseh to reach for excellence in endodontics and superior cleaning and disinfection methods for root canal therapy in his practice profile, titled, “Lights, camera, endo!” https://endopracticeus.com/allen-ali-nasseh-dds-mmsc/
Author Info
 Allen Ali Nasseh, DDS, MMSc, is an endodontist practicing in Boston Massachusetts and the CEO and President of Real World Endo® an education, innovation, and medical device company. Dr. Nasseh is a clinical advisor to NIH/NIDCR Consortium for Regenerative Sciences and the ADA Instruments and Materials Committee. He is an international speaker and a senior clinical instructor and lecturer at Harvard School of Dental Medicine and is on the editorial staff of several peer-reviewed journals and periodicals.
Allen Ali Nasseh, DDS, MMSc, is an endodontist practicing in Boston Massachusetts and the CEO and President of Real World Endo® an education, innovation, and medical device company. Dr. Nasseh is a clinical advisor to NIH/NIDCR Consortium for Regenerative Sciences and the ADA Instruments and Materials Committee. He is an international speaker and a senior clinical instructor and lecturer at Harvard School of Dental Medicine and is on the editorial staff of several peer-reviewed journals and periodicals.
Disclosure: Dr. Nasseh has helped develop many of the products and techniques discussed in this article and receives royalties from his developments and innovations.
References
- Zehnder M. Root canal irrigants. J Endod. 2006 May;32(5):389-398.
- Bergenholtz G. Assessment of treatment failure in endodontic therapy. J Oral Rehabil. 2016 Oct;43(10):753-758.
- Nasseh AA. Streamlining effective irrigation. Endodontic Practice US. 2022;15(3): 10-12.
- Haapasalo M, Shen Y, Wang Z, Gao Y. Irrigation in endodontics. Br Dent J. 2014 Mar;216(6):299-303.
- Wang Z, Shen Y, Haapasalo M. Effect of smear layer against disinfection protocols on Enterococcus faecalis-infected dentin. J Endod. 2013 Nov;39(11):1395-1400.
- Macedo RG, Herrero NP, Wesselink P, Versluis M, van der Sluis L. Influence of the dentinal wall on the pH of sodium hypochlorite during root canal irrigation. J Endod. 2014 Jul;40(7):1005-1008.
- Machado R, Rother A, Comparin D, Pawar AM, Matos FDS, Cunha TC, Alberton LR, Paranhos LR. Removal of the smear layer by passive and continuous ultrasonic irrigation: a scanning electron microscopy study. J Oral Res. 2021;10(6): 1-8.
- Al-Zuhair H, Su Z, Liu H, Wang Z, Haapasalo M, Hieawy A, Gao Y, Shen Y. Antimicrobial effects of agitational irrigation on single- and multispecies biofilms in dentin canals. 2023 Jan;111(1):49-56.
- Stojicic S, Zivkovic S, Qian W, Zhang H, Haapasalo M. Tissue dissolution by sodium hypochlorite: effect of concentration, temperature, agitation, and surfactant. J Endod. 2010 Sep;36(9):1558-1562.
- Clarkson RM, Kidd B, Evans GE, Moule AJ. The effect of surfactant on the dissolution of porcine pulpal tissue by sodium hypochlorite solutions. J Endod. 2012 Sep;38(9): 1257-1260.
- La Rosa GRM, Plotino G, Nagendrababu V, Pedullà E. Effectiveness of continuous chelation irrigation protocol in endodontics: a scoping review of laboratory studies. 2023 Jul.
- Andrabi SM, Kumar A, Mishra SK, Tewari RK, Alam S, Siddiqui S. Effect of manual dynamic activation on smear layer removal efficacy of ethylenediaminetetraacetic acid and SmearClear: an in vitro scanning electron microscopic study. Aust Endod J. 2013 Dec;39(3):131-136.
- Sheng X, Yu J, Liu H, Wang Z, Deng S, Shen Y. Dual effectiveness of a novel all-in-one endodontic irrigating solution in antibiofilm activity and smear layer removal. Front Bioeng Biotechnol. 2023 Aug 1;11:1254927.
- Retamozo B, Shabahang S, Johnson N, Aprecio RM, Torabinejad M. Minimum contact time and concentration of sodium hypochlorite required to eliminate Enterococcus faecalis. J Endod. 2010 Mar;36(3):520-523.
Stay Relevant With Endodontic Practice US
Join our email list for CE courses and webinars, articles and more..
