Dr. Hugo Sousa Dias illustrates how his MANI files provided efficient and time-saving biomechanical preparation in this clinical case.
Dr. Hugo Sousa Dias illustrates retreatment of a case with complex root canal anatomy
Introduction
It is well established that the success and predictability of root canal treatment to prevent or cure apical periodontitis is dependent upon accurate diagnosis and performing each stage of treatment to a high standard.1 The endodontic treatment failure is usually associated with insufficient disinfection of the root canal system (RCS), unfilled or inadequate root canal obturation, and defective coronal restoration.2 Endodontic retreatment is the primary therapeutic option in these cases and initially involves removal of the obturation material to allow thorough cleaning, disinfection, and shaping.3
Instrumentation during retreatment procedures can lead to changes in dentin volume and transportation of root canals. Transportation can result in ledging, zipping, and perforation, particularly in the apical third, and weakens the tooth structure.4 The ideal root canal preparation is one where the original canal morphology is maintained during the biomechanical preparation along with the development of flaring from coronal to the apical portion and preserving the apical foramen.5 However, the ideal root canal preparation may not be always possible due to the complexity of the root canal anatomy.6
Different root and root canal configuration types can be found in any group of teeth. Therefore, a thorough knowledge of their most common anatomic morphologies and variations may help clinicians detect those deviations during root canal therapy, enhancing the chance for successful treatment.7 Several studies have reported that maxillary premolars have a highly variable internal canal configuration. According to Martins, et al.,8 the prevalence of upper first premolars with one root is between 36.4%-83.2%, and the prevalence of type VI Vertucci (two separate canals leave the pulp chamber, merge in the body of the root, and redivide prior to the apex to exit as two distinct canals) is between 0.2%-12.3%.
One of the main factors related to these failures is that the lack of thorough knowledge of the morphological and anatomical variations of RCS can result in failure to identify all root canals or can result in the use of inadequate instrumentation, leading to endodontic treatment failure.9 Therefore, the first step in achieving a successful endodontic outcome is an exact evaluation of the RCS and its anatomical variations.10
This case report discusses the endodontic retreatment of a first upper premolar type VI Vertucci with MANI® GPR files for desobturation and JIZAI rotary endodontic system (MANI, Tochigi, Japan) for the shaping protocol.
MANI GPR (MANI, Inc. Utsunomiya, Japan) is a four-instrument system consisting of two stainless steel instruments to work in the straight segment of the canal (1S [70/0.04)] and 2S [50/0.04]), and two nickel-titanium instruments for the curved canal segment (3N [40/0.04] and 4N [30/0.04]).
JIZAI (MANI, Tochigi, Japan) is a NiTi rotary file system made of a proprietary heat-treated NiTi alloy with shape memory characteristics. JIZAI has an off-center quasi-rectangular cross section with a radial land on one of the short sides. The manufacturer claims that the radial land reduces screw-in forces, and that the off-centered design provides wide spaces for debris removal. For curved canals, a size 25 .04 taper instrument followed by a size 25 .06 taper instrument is used sequentially in a single length technique to the full working length. One study has reported that JIZAI exhibits flexibility and cyclic fatigue resistance comparable to HyFlex EDM® (Coltene-Whaledent, Allstätten, Switzerland), another contemporary single-length NiTi rotary system manufactured using electro-discharge machining followed by thermal treatment. The manufacturer recommends that JIZAI instruments can be operated at a maximum rotational speed of 500 rpm.11
Case report
A 42-year-old female patient was referred to the clinic with severe pain in the upper right first premolar teeth from a local dentist. The patient gave a history of pain for 3 months that aggravates when chewing and while sleeping and relieves after taking the medications. No significant medical history was observed.
The intraoral examination revealed a provisional restoration in tooth No 14. Pain on percussion was observed for tooth No.14. A intraoral periapical radiograph (IOPA) was advised to draw the final diagnosis and treatment plan. The IOPA revealed a periapical radiolucency in an endodontically treated tooth (No. 14). A final diagnosis of previously treated tooth with symptomatic apical periodontitis was confirmed, and the root canal retreatment was advised (Figure 1).
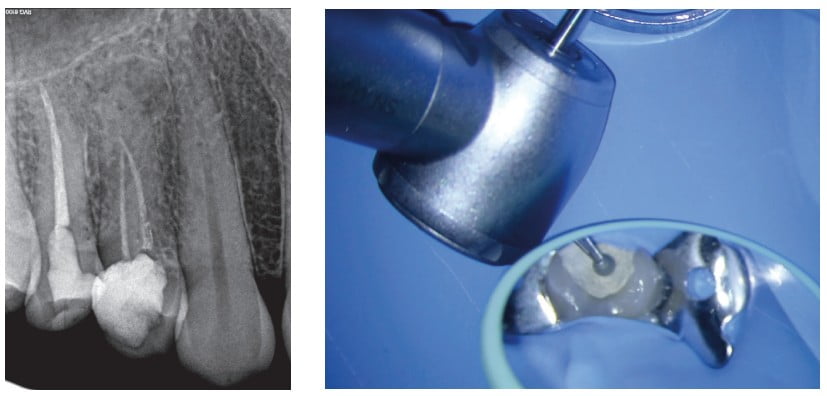
After administrating local anesthesia (2% lignocaine 1:200000 epinephrine), access cavity preparation was performed with BR-154 round bur (MANI, Tochigi, Japan) (Figures 2A and 2B). The pulp chamber was irrigated by following the standardized irrigation regimen of 5.25% of NaOCl. The desobturation was done with MANI GPR (MANI, Tochigi, Japan); gutta percha was removed using the 2S (50/0.04) instrument in continuous rotation at 1000 rpm and 2 Ncm in the coronal part. Then the 3N (40/0.04) instrument was used up to 2 mm short of the obturation material (Figure 3). Next, the patency of the root canals was determined using No. 8, No. 10, and No. 12 D-Finder files (MANI, Tochigi, Japan), and the working length (WL) was confirmed using a Electronic Apex Locator (Morita TriAuto ZX2, J. Morita, Japan).

Mechanical glidepath was done with JIZAI GLIDER (13.04) (MANI, Tochigi, Japan), according to company parameters (300 rpm, 1 Ncms). The shaping protocol was done with JIZAI (MANI, Tochigi, Japan) rotary files with a modification in the suggested protocol.

For coronal flaring JIZAI (MANI, Tochigi, Japan) 25.06 was used (Figure 4). After copious irrigation with 5.25% of sodium hypochlorite, it was used with the 25.04 up to the WL in both root canals (Figure 5), and the shaping protocol was finished with 25.06 (Figure 6).

The final irrigation protocol was done with 5.25% of sodium hypochlorite, 17% ethylenediaminetetraacetic acid and physiological saline with Endo1 (passive ultrasonic irrigation) (Woodpecker) (Figure 7).

The hydraulic condensation technique was performed using bioceramic sealer (CeraSeal, MetaBiomed) with 25.04 master cones (Figures 8 to 10). The pulp chamber was sealed with Ionoseal® (VOCO, Germany) (Figure 11), and a temporary restoration was made. The patient was referred to her dentist for the permanent coronal restoration.
The postoperative instructions were given to the patient and recalled after 3 months for evaluation.
Discussion
Due to the complexity of internal root canal anatomy, the development of new instruments, which are more flexible, more resistant to fracture, and effective in the shaping of root canals, is extremely important. It has been reported that the maintenance of the original canal shape and lack of canal aberrations are associated with the preservation of tooth structure and higher clinical success rates.12
Several novel thermomechanical processing and manufacturing technologies have been developed to optimize the microstructure of NiTi alloys to improve flexibility and fatigue resistance of endodontic instruments.13 Other recent developments in file design include an off-centered cross section. The principle of this design is to minimize the engagement between the file and the dentin of the canal wall, therefore decreasing the load on the file. Such a cross section also allows space for debris to accumulate between the flutes of the file, and it is driven in a coronal direction. It is anticipated that such a design will enhance cleaning of the root canal system due to efficient debris removal. The off-centered cross-sectional design also allows greater flexibility in the file. This is achieved as this file design creates a larger envelope of motion and will cut a larger preparation compared to a file with a conventional cross-sectional design. Therefore, a greater tapered preparation can be created with a file that has a smaller centered mass, which will mean the file is more flexible.1
According to Nakatsukasa, et al.,11 JIZAI (MANI, Tochigi, Japan) showed better centering ability. It also exhibited flexibility and cyclic fatigue resistance similar to EDM, maintaining a canal curvature, and generated smaller torque and screw-in force than other files. Accurate knowledge of root canal morphology and its anatomical variations are essential for successful root canal treatment.6 Teeth with straight root canals are very rare to observe in endodontics as most of the teeth tend to exhibit some sort of curvature and multiple planes of deviations along the course of the root canal length.15 The endodontic complications — e.g., the ledge formations, canal blockages, root canals perforations, and apical transportations — are usually observed with the improper handling of the instruments or improper techniques of instrumentations in these clinical cases.16
Many technological advancements have been made to preserve the original canal curvature and to prevent inadvertent instrument fracture, including changes to the cross-sectional design,17 motion,18 and metallic property.19 In particular, heat treatment changes the phase transformation temperature of the NiTi alloy, which results in the growth of soft and ductile phases — i.e., the martensite phase and R-phase, thereby enhancing the fracture resistance and flexibility.20
This clinical case is well managed; and with the use of adequate instruments, the root canal anatomy can be respected, and all mechanical and biological goals can be accomplished.
Conclusion
Ongoing development in instrumentation techniques is making endodontics easier, and operators can now achieve the desired canal shape more quickly. Furthermore, with various root canal preparation systems now available, canals that may once have been deemed too difficult to negotiate and prepare are now more manageable. The appropriate root canal instrumentation techniques need to be selected based on the root canal anatomy, calcifications, and economic factors.
The JIZAI rotary instrumentation has shown an efficient and time-saving biomechanical preparation in this clinical case and thus is indicated for safe and efficient biomechanical preparations in curved and constricted root canal systems.
To see a video of the procedure visit: https://m.youtube.com/watch?v=zW3a4p5V5xo&feature=youtu.be
 Hugo Sousa Dias, DDS, received his Doctor of Dentistry in 2008 from the Universidade Fernando Pessoa – Porto, Portugal. In 2015, he completed his postgraduate program in endodontics at University of Lisbon – School of Dentistry, Portugal. He lectures and leads hands-on courses worldwide. He is the founder of Hugo Sousa Dias & Friends webinar sessions. His areas of special interest follow: pulp canal obliterations, guided endodontics, separated instruments retrieval, instrumentation and obturation, retreatments, MTA and other bioceramics, apical microsurgery, and regenerative endodontics. Dr. Dias is in private practice limited to endodontics in Porto, Portugal.
Hugo Sousa Dias, DDS, received his Doctor of Dentistry in 2008 from the Universidade Fernando Pessoa – Porto, Portugal. In 2015, he completed his postgraduate program in endodontics at University of Lisbon – School of Dentistry, Portugal. He lectures and leads hands-on courses worldwide. He is the founder of Hugo Sousa Dias & Friends webinar sessions. His areas of special interest follow: pulp canal obliterations, guided endodontics, separated instruments retrieval, instrumentation and obturation, retreatments, MTA and other bioceramics, apical microsurgery, and regenerative endodontics. Dr. Dias is in private practice limited to endodontics in Porto, Portugal.
Dr. Dias is also the Director of the Endodontic Master Program at Foramen Dental Education – Porto, Portugal, since 2015. In 2019, he started a new teaching project, Side By Side Custom Endodontic Made Programs for individualized training in endodontics. He is a founder and active member of the Portuguese Group For Endodontic Study, organizing study club sessions in different parts of Portugal. Dr. Dias is a board member of the Portuguese Endodontic Society and a member of European Society Endodontology. He is an invited professor of Endodontic Post-Graduation Programs at University of Lisbon – School of Dentistry, CESPU University, and University of Porto – School of Dentistry. He is a member of the Clinical Masters Network and has published clinical reports in Roots Magazine, Clinical Masters Magazine and Saude Oral Magazine.
Disclosure: Dr. Dias is a key opinion leader for KaVo Kerr (2013-2017); Mani, Inc. (since 2017); Septodont (since 2018); and Karl Kaps GMBH & Co. KG (since 2021).
- Tomson PL, Simon SR. Contemporary cleaning and shaping of the root canal system. Prim Dent J. 2016;5(2):46-53.
- Rödig T, Reicherts P, Konietschke F, et al. Efficacy of reciprocating and rotary NiTi instruments for retreatment of curved root canals assessed by micro-CT. Int Endod J. 2014;47(10):942-948.
- Stabholz A, Friedman S. Endodontic retreatment: case selection and technique — part 2: treatment planning for retreatment. J Endod. 1988;14(12):607-614.
- Ganesh A, Venkateshbabu N, John A, Deenadhayalan G, Kandaswamy D. A comparative assessment of fracture resistance of endodontically treated and re-treated teeth: an in vitro study. J Conserv Dent. 2014;17(1):61-64.
- Peters OA. Current challenges and concepts in the preparation of root canal systems: A review. J Endod. 2004;30(8):559-567.
- Estrela C, Bueno MR, Sousa-Neto MD, Pécora JD. Method for determination of root curvature radius using cone-beam computed tomography images. Braz Dent J. 2008;19(2):114-118.
- Karabucak B, Bunes A, Chehoud C, Kohli MR, Setzer F. Prevalence of apical periodontitis in endodontically treated premolars and molars with untreated canal: a cone-beam computed tomography study. J Endod. 2016;42(4):538-541.
- Martins JNR, Marques D, Silva EJNL, Caramês J, Versiani MA. Prevalence Studies on Root Canal Anatomy Using Cone-beam Computed Tomographic Imaging: A Systematic Review. J Endod. 2019;45(4):1-15.
- Vertucci FJ. Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol. 1984;58(5):589-599.
- de Pablo OV, Estevez R, Péix Sánchez M, Heilborn C, Cohenca N. Root anatomy and canal configuration of the permanent mandibular first molar: a systematic review. J Endod. 2010;36(12):1919-1931.
- Nakatsukasa T, Ebihara A, Kimura S, et al. Comparative evaluation of mechanical properties and shaping performance of heat-treated nickel titanium rotary instruments used in the single-length technique. Dent Mater J. 2021;40(3):743-749
- Gutmann JL, Gao Y. Alteration in the inherent metallic and surface properties of nickel-titanium root canal instruments to enhance performance, durability and safety: a focused review. Int Endod J. 45(2):113-128
- Azim AA, Griggs JA, Huang GT. The Tennessee study: factors affecting treatment outcome and healing time following nonsurgical root canal treatment. Int Endod J. 49(1)6-16.
- Estrela C, Bueno MR, Couto GS, et al. Study of root canal anatomy in human permanent teeth in a subpopulation of Brazil’s center region using cone-beam computed tomography – Part 1. Braz Dent J. 2015;26(5):530-536
- Ruddle C. Cleaning and shaping the root canal system. In: Cohen S, Burns RC, (eds.) Pathways of the Pulp. 8th ed. Mosby; 2002.
- Patnana AK, Kanchan T. Endodontic management of curved canals with ProTaper Next: A case series. Contemp Clin Dent. 2018;9(suppl 1):S168-S172.
- Kyaw Moe MM, Jo HJ, Ha JH, Kim SK. Root canal shaping effect of instruments with offset mass of rotation in the mandibular first molar: a micro-computed tomographic study, J Endod. 2018;44(5):822-827.
- Kimura S, Ebihara A, Maki K, et al. Effect of optimum torque reverse motion on torque and force generation during root canal instrumentation with crown-down and single-length techniques. J Endod. 2020;46(2):232-237.
- Shen Y, Zhou HM, Zheng YF, Peng B, Haapasalo M. Current challenges and concepts of the thermomechanical treatment of nickel-titanium instruments. J Endod. 2013;39(2):163-172.
- Zupanc J, Vahdat-Pajouh N, Schäfer E. New thermomechanically treated NiTi alloys — a review. Int Endod J. 2018;51(10):1088-1103.
Stay Relevant With Endodontic Practice US
Join our email list for CE courses and webinars, articles and more..
