Dr. L. Stephen Buchanan shares his view of the importance of maintaining structural integrity and practicing minimally invasive endodontics.
Dr. L. Stephen Buchanan discusses approaching zero loss of structural integrity during RCT
Mentioning the term “minimally invasive endodontics” (MIE) invites a wide a range of emotional responses and definitions from endodontic specialists worldwide. “Ninja” access cavity preparations have bedeviled us as we’ve struggled to work through their compromised convenience form. We’ve lost heart muscle in frustration with the challenges of irrigating and cone fitting 15-.03 root canal shapes. Yet MIE is here to stay. Why? Because preserving our patient’s tooth structure during RCT is a virtuous objective as well as being the best argument against replacement of teeth with implants rather than saving them with RCT.
What does MIE even mean? Regarding any specific RCT case — in my opinion — MIE means whatever the treating DDS says it is! If you weren’t holding the file, you aren’t the MIE shot caller. This is the number one thing to keep in mind when getting small — if the case fails because the convenience form of a Ninja access prep was inadequate, did we really preserve tooth structure? Also, within the skill level of a given DDS doing RCT, MIE will mean different things in different cases. When calcified canals elude us, when interocclusal distances are small, and even when patients are being jerks, if it’s necessary to cut a bit bigger access cavity to get the case done successfully, that is yours to decide and work through.
Don’t forget that at any time during the procedure, if it’s not working, stop, refine the entry path of the access line angle, and continue on. This is experienced most often during cone fitting because it requires a larger access opening to cement GP cones in all the canals at once than it does to instrument and irrigate them.
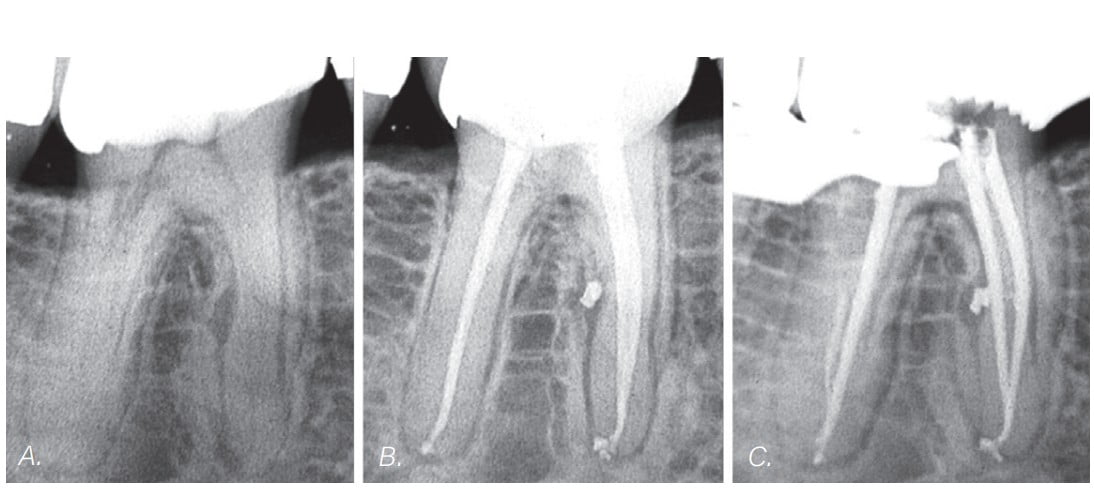
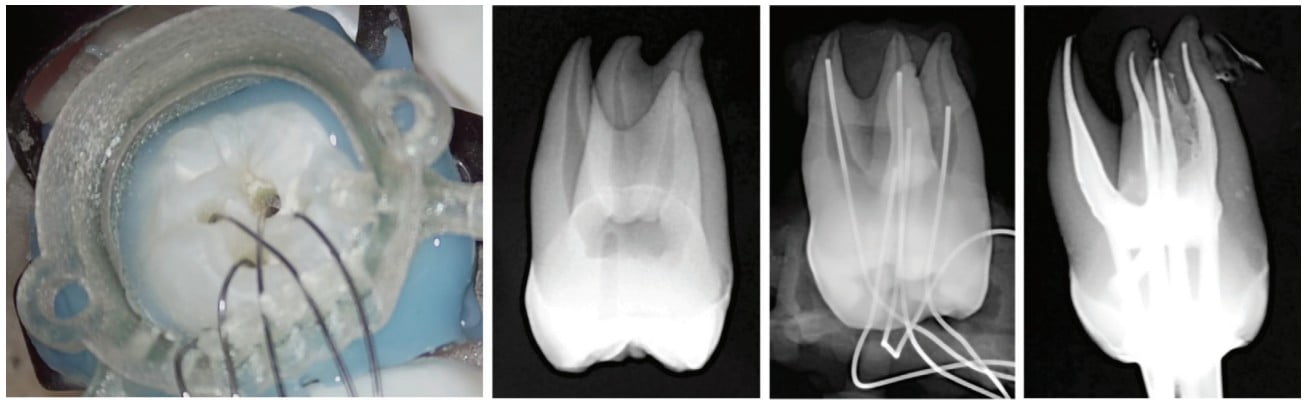
While MIE may be a relatively new trend to many endodontists, it isn’t new to endodontics. The case shown in Figure 1 was treated shortly after the advent of rotary shaping files, demonstrating the shape of things to come in both conceptual and procedural terms. An interesting sidenote is that all three of the canals in Figure 1 were single-file shapes, cut with rotary rather than reciprocating motion. The case in Figure 2 shows the results of the following 20-plus years of MIE development— a case with dilacerated canal curvatures completely negotiated and shaped with a single rotary file in each canal.

The case in Figure 2 was completely negotiated with miniKUT EZP 15-.05 rotary negotiating files (PlanB Dental, Goletta, California) despite the dramatic canal curvatures encountered. This was a beautiful demonstration of the efficacy of rotary negotiation because after I determined that I was unable to reach the DB terminus using No. 06, No. 08, and No. 10 SS K-Files by hand, the miniKUT 15-.05 EZP rotary file cut to length in two passes! That is so counterintuitive considering our common belief that hand files are more facile than rotary files when making our way to length the first time. The fact of the matter is that with the right file tip geometry (Figure 3), rotary files are able to bump and bounce past canal impediments that stainless steel hand files will engage in every time.

When powered by a cordless endodontic handpiece containing an integrated apex locator (Figure 4), rotary negotiation with miniKUT EZP files can easily save 10-30 minutes of treatment time in a difficult molar.

One of the coolest aspects of minimally invasive endodontic concepts is that as soon as clinicians accept the reality that tiny canal shapes can be adequately cleaned with irrigants, the number of instruments needed to complete instrumentation drops to one or two files per canal — including negotiation — without the need for overpriced rotary or reciprocation NiTi files.
How do we irrigate MIE canal preparations? There are several high-tech irrigation methods that can do the job, including multisonic irrigation (GentleWave® by Sonendo®, Laguna Hills, California) and YSGG laser cavitation (WaterLase® by Biolase®, Foothill Ranch, California). Those methods are fun and effective for high-tech early adopters but require a capital investment of $40K to $80K, plus per/case fees, plus maintenance fees, plus the cost of rapid obsolescence. Low-tech methods such as continuous irrigation with a conventional syringe and a safe-ended cannula can be just as effective if given enough time to definitively irrigate multicannular teeth — one canal at a time. Better yet, using a negative-pressure, multicannular irrigation device, e.g, PulpSucker (PlanB Dental), means you can have a cappuccino while it runs by itself after staging is completed (Figure 5).
With that said, how do we approach zero loss of structural integrity during RCT?
Keep in in mind the following thoughts:
- We do not clean canals with files; we use files to cut the shape in root canals needed to adequately clean and fill them in three dimensions. That’s it. Corollary to No. 1: When canals present with adequate shape, don’t cut any dentin. Just irrigate the snot out of the RCS, and stuff it. These opportunities are most commonly seen in young patients with pulpitic teeth with recently completed root formation.
- Access openings as small as 1 mm in diameter are large enough to provide adequate convenience form as long as they are angled such that files do not bend to enter canal orifices. When operating at this level, it is very helpful to use dynamic guidance systems like X-Guide® (X-Nav Technologies).
- The ideal MIE access path is often through pre-existing decay and restorations where little or no further tooth structure needs to be cut to accomplish the RCT. While I prefer to treat molars through a mesially tipped access cavity preparation, I will do the more conservative but difficult thing by operating through the distal of a tooth when it has been destroyed by caries.
- Enlarging the coronal halves of canals beyond 0.8 mm to 1.0 mm does not improve irrigation efficacy at all.
- Enlarging the coronal halves of canals beyond 0.8 mm to 1.0 mm does not improve obturation results either.
When Dr. Herbert Schilder wrote that canals should have continually tapering root canal shapes, he was addressing clinicians during an era of rigid stainless steel files and pluggers, and we needed those larger coronal shapes to accomplish our clinical objectives in the apical third. Today most of these issues are moot — we now have hyperflexible files, irrigating cannulas, carriers, and electric heat pluggers — so it is senseless to continue to advocate cutting more dentin for no clinical advantage. Yet many endodontists have not received the memo and still associate big access cavities and boofy coronal canal shapes as the “Look” of well-done RCT when they are actually just mementos of no longer relevant endodontic history.
*The cases were all treated by the author.
Endodontic Practice US readers appreciate Dr. Buchanan’s insights on structural integrity. Read about his journey to becoming a top educator here: https://endopracticeus.com/l-stephen-buchanan-dds/
 Stephen Buchanan, DDS, FICD, FACD, Dipl. ABE, has been lecturing and teaching hands-on endodontic continuing education courses for over 30 years, both in his state-of-the-art training facility in Santa Barbara, California, as well as in dental schools and at meetings around the world. He currently serves as a part-time faculty member in the endodontic departments at the University of the Pacific’s Arthur Dugoni School of Dentistry and the University of California at Los Angeles as well as being the Endodontic Advisory Board Member to the Academy of General Dentistry. Dr. Buchanan is nationally and internationally known for his 50-plus endodontic procedural articles as well as his expertise in the research and development of new endodontic technology, instruments, and techniques. He is a Diplomate of the American Board of Endodontists, a Fellow of the International and American College of Dentists. Dr. Buchanan also maintains a private practice limited to Endodontics in Santa Barbara, California.
Stephen Buchanan, DDS, FICD, FACD, Dipl. ABE, has been lecturing and teaching hands-on endodontic continuing education courses for over 30 years, both in his state-of-the-art training facility in Santa Barbara, California, as well as in dental schools and at meetings around the world. He currently serves as a part-time faculty member in the endodontic departments at the University of the Pacific’s Arthur Dugoni School of Dentistry and the University of California at Los Angeles as well as being the Endodontic Advisory Board Member to the Academy of General Dentistry. Dr. Buchanan is nationally and internationally known for his 50-plus endodontic procedural articles as well as his expertise in the research and development of new endodontic technology, instruments, and techniques. He is a Diplomate of the American Board of Endodontists, a Fellow of the International and American College of Dentists. Dr. Buchanan also maintains a private practice limited to Endodontics in Santa Barbara, California.
Disclosure: Dr. Buchanan is a stockholder of Sonendo®; he is the inventor and owner of the IP associated with the closed-system, negative pressure, positive outflow irrigation (PulpSucker) device described in this article, and he is PlanB Dental’s Clinical Director.
Stay Relevant With Endodontic Practice US
Join our email list for CE courses and webinars, articles and more..
