Dr. Lauren Tink shows how using the GentleWave System on a pediatric patient can reduce the challenges of pediatric patients in the endodontic office.
Dr. Lauren Tink treats an anxious pediatric patient using an efficient treatment
Introduction
Recent advancements in endodontic techniques have revolutionized our ability to manage pediatric patients with complex cases. Traditionally, cases with wide open apices presented significant challenges. These cases often required multiple visits in order to achieve optimal outcomes.
However, contemporary approaches have provided more efficient treatment options, leading to improved clinical results and patient satisfaction.
Apexification has been the treatment of choice for teeth with open apices, aiming to induce the formation of an artificial apical barrier. While effective, apexification has its limitations as there is no potential for further root development.1 The emergence of regenerative endodontics has offered a paradigm shift in the management of these cases.2 This technique not only addresses the underlying pathology but also allows for continued root growth, ultimately leading to a more functional and resilient dentition.3
The implementation of traditional pulpal regeneration protocols in pediatric patients can be challenging, especially in cases with limited cooperation. Conventional approaches often require multiple visits,4 increasing the burden on both the patient and the clinician.
Single visit regenerative endodontics, coupled with advanced disinfection techniques, have emerged as a promising solution. This approach requires fewer visits, allows for enhanced disinfection, and promotes optimal blood clot formation in the canal. By eliminating the need for multiple visits, single visit regenerative endodontics offers a patient-centered approach that prioritizes both clinical outcomes and patient comfort.
In this case report, we present a 10-year-old patient with a wide open apex and a dens evaginatus.5 This case was successfully managed with single visit regenerative endodontics using the GentleWave® System (Sonendo®).6 The outcomes demonstrate not only the feasibility but also the efficacy of this approach in achieving favorable clinical and radiographic results in pediatric patients.
Case report
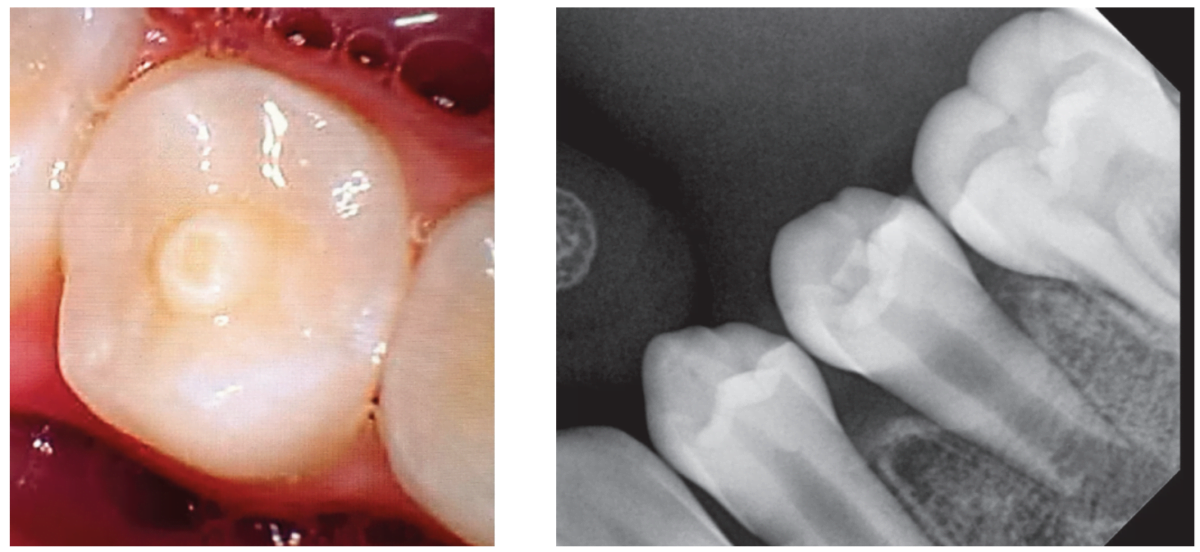
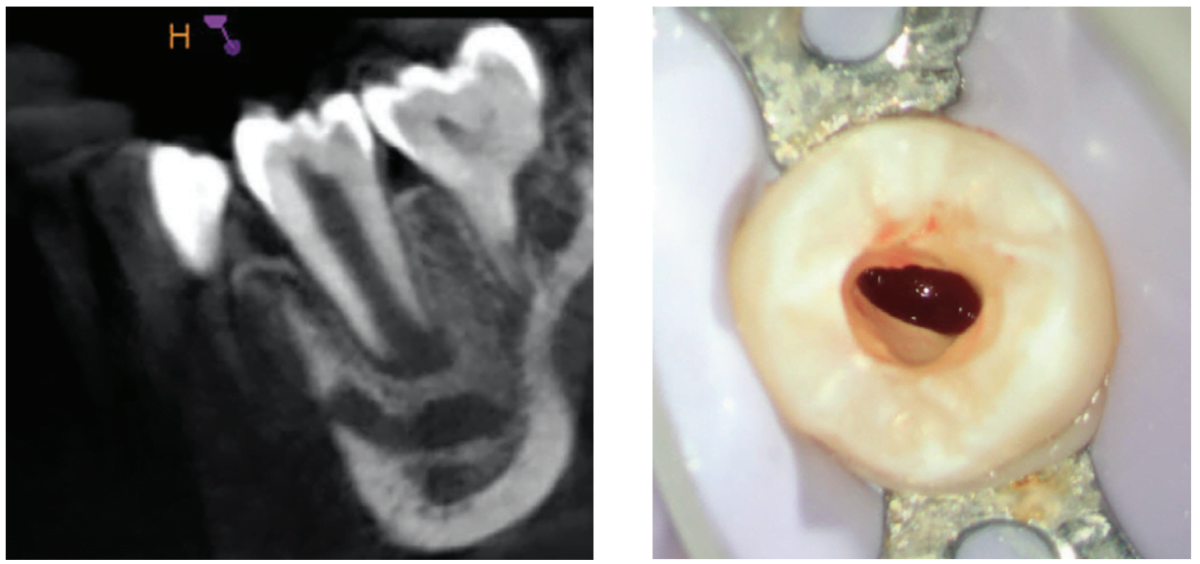
A 10-year-old female patient with a history of swelling and pain associated with tooth No. 20 was referred to our office. The patient exhibited severe dental anxiety. Upon clinical evaluation, a dens evaginatus was noted on the occlusal surface of the tooth (Figure 1). The tooth was sensitive to percussion, palpation, and bite stick while cold testing yielded no response. A periapical radiograph and CBCT scan (Carestream 9600) revealed a wide open apex and evidence of apical periodontitis, leading to the diagnosis of a necrotic pulp and symptomatic apical periodontitis of tooth No. 20 (Figures 2 and 3).
Given the presence of a wide open apex, traditional root canal therapy was not possible in this case. Treatment options such as apexification and regenerative endodontics were discussed along with the risks and benefits of both modalities. With apexification, placing the apical plug would present a challenge since there would be a risk of extruding the material past the apex. In addition, this option would present no opportunity for increasing the root width and length. For these reasons, it was determined that pulpal regeneration would be the ideal approach. The goals of the pulpal regeneration procedure would include facilitating root formation while eliminating apical periodontitis and achieving an asymptomatic and functional outcome for the patient. Traditionally, pulpal regeneration would be completed over the course of two visits with interim calcium hydroxide or triple antibiotic paste. However, this 10-year-old patient was severely anxious. Her parents requested for her to be treated under IV sedation. By maintaining the traditional protocol for pulpal regeneration, the patient would have to undergo IV sedation twice at two separate visits.
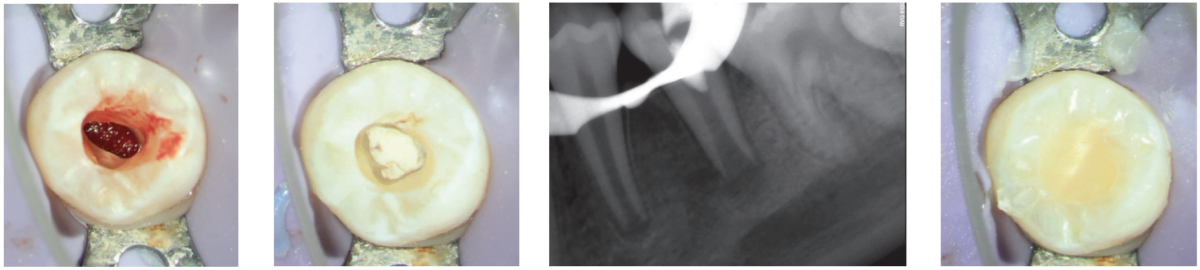
An alternative approach of single visit regenerative endodontics was employed utilizing the GentleWave system to facilitate disinfection and blood clot formation. After the IV was placed, local anesthesia was administered using 3% mepivacaine. No vasoconstrictor was used so as not to inhibit blood flow to the tooth. After isolating with a rubber dam, the tooth was accessed. A necrotic pulp was noted. No endodontic files were used for instrumentation. Flowable dam material (EndoSequence®, Brasseler USA) was used to build a platform and create a seal for the GentleWave CleanFlow™ procedure instrument (Sonendo). The full GentleWave cycle was run using NaOCl and EDTA as irrigants with a final water flush. Once the platform was removed, bleeding was immediately noted in the canal (Figure 4). A microsuction tip was used to control the bleeding to below the level of the CEJ. A piece of collagen tape (HeliCote® Collagen Dressing by Integra Miltex) was placed over the blood clot (Figure 5). Bioceramic putty (EndoSequence BC RRM Fast Set Putty) was placed on top of the collagen tape (Figures 6 and 7). The chamber was then etched and bonded and restored using Luxacore build up material (LuxaCore Z Dual Cure) and light-cured resin composite (Clearfil Majesty™ Composite, Kuraray) (Figures 8 and 9).
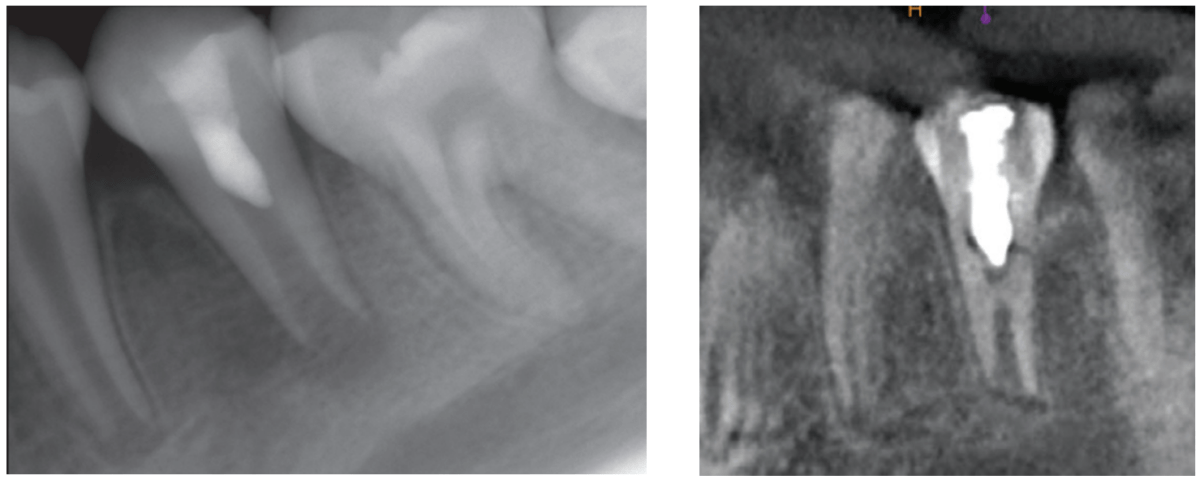
The patient was recalled 6 months later and showed promising results. She was asymptomatic and functional. The CBCT scan showed no evidence of apical periodontitis (Figure 10). Thickening of the radicular walls was noted, and a calcific barrier was noted to be forming mid-root. She will continue to be recalled in another 6 months to continue monitoring the healing of this case.
Summary
In conclusion, this case report highlights the successful management of an anxious pediatric patient with a wide open apex using single visit regenerative endodontics, incorporating the GentleWave procedure. By circumventing the need for multiple visits and integrating advanced disinfection techniques, this approach not only expedited treatment but also optimized disinfection and facilitated blood clot formation in the canal. The favorable clinical and radiographic outcomes observed underscore the efficacy and feasibility of single visit regenerative endodontics as a patient-centered approach for addressing challenging cases in pediatric patients with limited cooperation and severe dental anxiety.
Read Dr. Scott Hetz’s experience with the GentleWave in his article, “Healing and long-term results with the GentleWave® Procedure,” at https://endopracticeus.com/healing-and-long-term-results-with-the-gentlewave-procedure/.
 Lauren Tink, DMD, was born and raised in Montreal, Canada. She attended McGill University and earned her doctoral degree in 2014. Following graduation, Dr. Tink moved to New York City and furthered her training at NYU Lutheran Medical Center’s Advanced Education in General Dentistry residency program. Subsequently, she attended Nova Southeastern University where she earned her postdoctorate degree in Endodontics. During her training at Nova, Dr. Tink participated in a surgical externship in Barcelona, Spain at the Universitat Internacional de Catalunya, performing a variety of specialized surgical procedures. She is currently in private practice at Weston Endodontic Care in Weston, Florida.
Lauren Tink, DMD, was born and raised in Montreal, Canada. She attended McGill University and earned her doctoral degree in 2014. Following graduation, Dr. Tink moved to New York City and furthered her training at NYU Lutheran Medical Center’s Advanced Education in General Dentistry residency program. Subsequently, she attended Nova Southeastern University where she earned her postdoctorate degree in Endodontics. During her training at Nova, Dr. Tink participated in a surgical externship in Barcelona, Spain at the Universitat Internacional de Catalunya, performing a variety of specialized surgical procedures. She is currently in private practice at Weston Endodontic Care in Weston, Florida.
Disclosure: Dr. Tink reports no financial or other interests regarding any of the products mentioned in this article.
- Rafter M. Apexification: a review. Dent Traumatol. 2005 Feb;21(1):1-8.
- Diogenes A, Ruparel NB, Shiloah Y, Hargreaves KM. Regenerative endodontics: A way forward. J Am Dent Assoc. 2016 May;147(5):372-380.
- Lin J, Zeng Q, Wei X, Zhao W, Cui M, Gu J, Lu J, Yang M, Ling J. Regenerative Endodontics Versus Apexification in Immature Permanent Teeth with Apical Periodontitis: A Prospective Randomized Controlled Study. J Endod. 2017 Nov;43(11):1821-1827.
- American Association of Endodontists. AAE Clinical Considerations for a Regenerative Procedure: Revised 5/18/2021. https://www.aae.org/specialty/wp-content/uploads/sites/2/2021/08/ClinicalConsiderationsApprovedByREC062921.pdf. Accessed May 17, 2024.
- Lerdrungroj K, Banomyong D, Songtrakul K, Porkaew P, Nakornchai S. Current Management of Dens Evaginatus Teeth Based on Pulpal Diagnosis. J Endod. 2023 Oct;49(10):1230-1237.
- Sigurdsson A, Garland RW, Le KT, Woo SM. 12-month Healing Rates after Endodontic Therapy Using the Novel GentleWave System: A Prospective Multicenter Clinical Study. J Endod. 2016 Jul;42(7):1040-1048.
Stay Relevant With Endodontic Practice US
Join our email list for CE courses and webinars, articles and more..
