Extra canals and roots in certain teeth can compromise effective obturation techniques. This study reaffirms the importance of techniques that improve diagnosis.
 A study by Jessica Monteiro Mendes, Cristiane Melo Caram, Alexia da Mata Galvão, Nayara Rodrigues Nascimento Oliveira, Gisele Rodrigues da Silva, and Maria Antonieta Veloso Carvalho de Oliveira reaffirms the importance of techniques that improve the quality of endodontic diagnosis
A study by Jessica Monteiro Mendes, Cristiane Melo Caram, Alexia da Mata Galvão, Nayara Rodrigues Nascimento Oliveira, Gisele Rodrigues da Silva, and Maria Antonieta Veloso Carvalho de Oliveira reaffirms the importance of techniques that improve the quality of endodontic diagnosis
Abstract
The aim of this study is to evaluate the prevalence of extra roots and canals in the first and second lower molars over a 10-year period and correlate their occurrence with the patient’s age and gender, treatment type, tooth type, and the use of operating microscope. For this study, 519 dental records and their digital radiographs (550 teeth) were analyzed and classified into four groups. The prevalence of an extra canal in the distal root, an extra canal in the mesial root, and an extra root were 39.65%, 2.90%, and 3.64%, respectively. Gender and treatment type were not statistically significant. The extra canals of the distal root are more common than the extra canals and extra roots of the distal root, and it was most frequent in younger (<40 years old) patients and in first molars. The operating microscope improved the identification of extra canals in the mesial root.
Introduction
The success of endodontic treatment is directly related to the location, instrumentation, and cleaning of all root canals, which can reduce bacteria and optimize the conditions needed for an effective obturation technique.1 Knowledge of internal and external root anatomy is fundamental for successful endodontic practices.2 Molars are anatomically complex and, therefore, have been the subject of numerous studies.3,4,5 Mandibular molars usually have two mesial root canals plus one distal root canal — called mesiobuccal, mesiolingual, and distal — but may also have fused roots or extra roots, isthmuses, and extra canals. The prevalence of the radix root is directly related to ethnicity, occurring in 3.4% to 6.8% of Caucasians6,7 and 21% to 24.5% in populations of Mongolian origin.8 The isthmus has a prevalence of 64.7% to 87%,9,10 while the middle mesial canal (MM) has a prevalence of 14.7%10 to 45.6%.11
The prevalence of anatomical variations in mandibular molars has been studied in relation to patient type (gender and age), tooth type (first or second mandibular molars),12 crown aspect and pulp chamber floor,10,13,14 root canal compliance/morphology,9,14,15 and the influence of complementary tests, technologies, and instrumentation techniques.9,10,11,12
Some studies have analyzed the prevalence and/or anatomy of these anomalies in a Brazilian population16,17,18,19 but have not correlated anatomical variations with patient and treatment factors. Therefore, the present study evaluates the prevalence of extra roots and canals in the first and second mandibular molars over a 10-year period of endodontic treatment and correlated their occurrence with factors such as patient age and gender, treatment type, tooth type, and the use of operating microscope.
Material and methods
Clinical and radiographic data from 519 dental records (550 teeth) were analyzed after receiving approval from the Research Ethics Committee of the Uberlândia Federal University (#1603416). The medical records belonged to patients attended from 2009 to 2019 at a private clinic (EndoMais, Uberlândia, Minas Gerais, Brazil) and by a single, experienced operator using standardized techniques. Only cases of endodontic treatment or retreatment on the first or second mandibular molars were included, while cases that were incomplete by December 2019 were excluded.
The following data was collected from digital files (ProDent® Dental Software, HartSystem, Blumenau, Santa Catarina, Brazil): number of canals treated, patient age (less or more than 40 years old), patient gender (male and female), tooth type (first or second molar), treatment type (treatment or retreatment), and the use of an operating microscope. The microscope used was a model MC12 DFV (D. F. Vasconcelos, Valença, RJ, Brazil). It was used in every case since 2015. The canal location (mesial, distal, buccal, and lingual) was determined by using clinical data and digital radiographs from all treatment stages (FONA Sensor and CDR DICOM Software, Schick, Dentsply Sirona, São Paulo, Brazil).
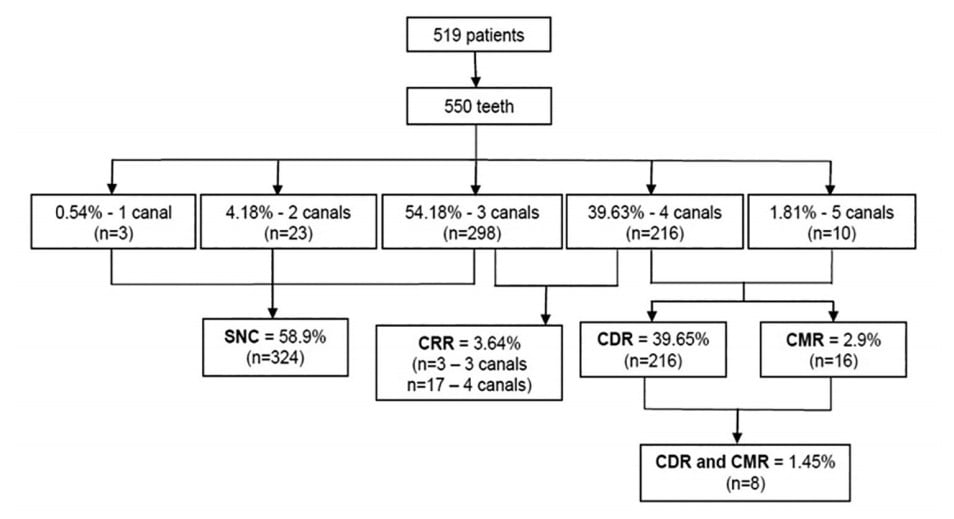
After data collection, these teeth (n = 550) were classified into four groups according to canals and roots:
- SNC group: teeth with a standard number of canals (one to three canals)
- CDR group: teeth with an extra canal in the distal root
- CRM group: teeth with an extra canal in the mesial root
- CRR group: teeth with canal in the radix
The chi-square test was used to determine the prevalence of anatomical abnormalities in the mandibular molars relative to patient age, gender, treatment type, tooth type, and the influence of operating microscopy. The analysis was based on presence of absence of the following:
- an extra canal in the mesial root
- an extra canal in the distal root
- an extra root
The data was analyzed using SigmaPlot 12.0 (Systat Software, Inc., Chicago, Illinois) at a significance level of 5%.
 Results
Results
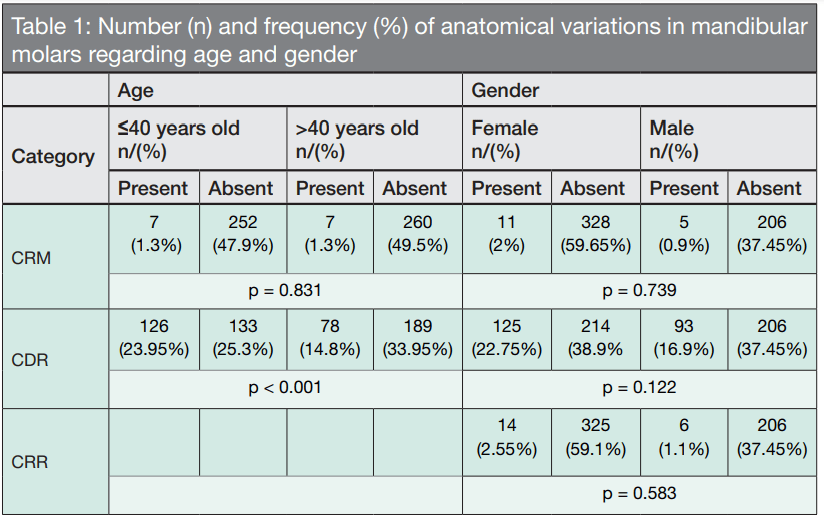
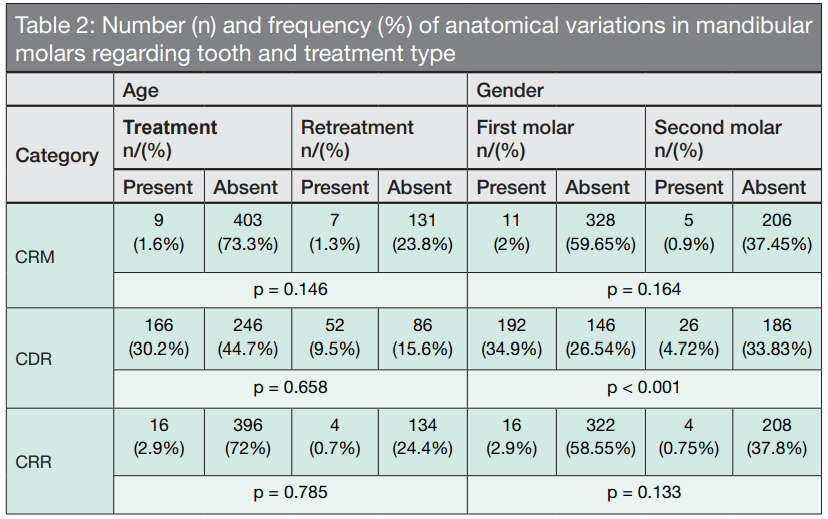
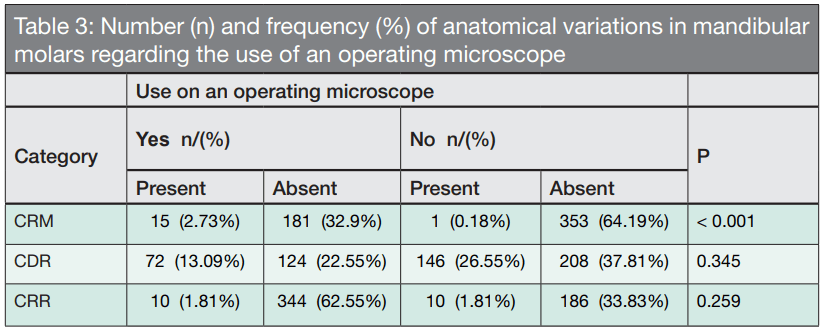
The results of the number and percentage of extra canals and roots in the mandibular molars are shown in Figure 1. Statistical differences regarding age (Table 1) were only found in the CDR group, which showed a higher frequency of extra canals in patients under 40 years old (p <0.001). Teeth with extra roots (CRR group) were not analyzed relative to age, as this variable does not vary over time. Statistically significant differences were not found regarding gender (Table 1) or treatment type (Table 2). However, the presence of an extra canal in the distal root of the first molar was statistically higher in the CDR group (Table 2). The operating microscope (Table 3) was a determining factor in increasing the ability to locate extra canals in the mesial root of the CRM group.
 Among the 16 teeth with an extra canal in the mesial root (CRM group), one was classified as “independent” (6.25%), one was “fin” (6.25%), and 14 were “confluent” (87.5%). Six of the cases with confluent anatomy had a mesiolingual canal, five had a mesiobuccal canal, and three had both. Sixteen of the teeth that had an extra root were entomolaris, while four were paramolaris.
Among the 16 teeth with an extra canal in the mesial root (CRM group), one was classified as “independent” (6.25%), one was “fin” (6.25%), and 14 were “confluent” (87.5%). Six of the cases with confluent anatomy had a mesiolingual canal, five had a mesiobuccal canal, and three had both. Sixteen of the teeth that had an extra root were entomolaris, while four were paramolaris.
 Discussion
Discussion
The inability to locate root canals may result in microbial material within the tooth, which may lead to apical periodontitis and a greater risk of failure.1 The most prevalent anatomical variation found in the 550 teeth analyzed in the present study was the extra canal in the distal root, followed by extra root and extra canal in the mesial root. The extra canal in the distal root — the most prevalent anatomical variation (25.5%) found in the mandibular molars — had been higher in first molars (34.9%). Similarly, Estrela, et al.,20 found that 51% of the first molars analyzed by cone beam computed tomography had four canals but did not specify whether the extra canal was distal or mesial. However, the microscopy did not influence the ability to identify these extra canals in the distal root — perhaps extra canals on distal roots are easy to locate in the pulp chamber floor when the endodontic access is adequate. Usually, the entrance of the distal canal is centralized between buccal and lingual walls. However, if this entrance is located to lingual or buccal, the existence of another root canal is highly probable.2 Extra canals in the distal root are more prevalent in patients younger than 40 years old. This may be related to aging, which causes alterations in root canal conformation due to the deposition of tertiary dentin. This deposition is in turn due to small daily occlusal traumas and pathological stimuli such as caries or dental erosion, which obliterate root canals as a defense form.21
Our study shows that the occurrence of an extra root, called a radix, is not influenced by patient age, tooth type, or the use of an operating microscope. The radix can be found in both first and second mandibular molars but is more prevalent in first molars.8,22 This root is classified as entomolaris when located lingually23 and paramolaris when located buccally.24 Prevalence is highly related to ethnicity, which hinders analysis in an ethnically diverse Brazilian population.18 Studies using radiographic analysis7 have shown a 2.8% to 4.2% prevalence in a Brazilian population, while studies using cone beam computed tomography have shown a prevalence of 2.58%16 or a total absence.18
The extra canal in the mesial root, referred to as a middle-mesial canal9,10,11,12,15,17 or an accessory mesial canal,25,26 is located between the mesiobuccal (MB) and mesiolingual (ML) canals. The entrance of this canal may be located anywhere between the pulp chamber floor to 2.0 mm below this limit.11 Studies show a prevalence of 14.7%,10 18.6%,17 and even 46.2%,11 using tomography, microtomography and operating microscopy, respectively. The middle-mesial (MM) canals can be classified as “independent” when they are separate from the pulp chamber floor to the apical foramen; “fin” when the MM joins the MB and/or the ML at some point and has separate foramens; and “confluent” when the MM has a separate entrance (or not) from that of the canals and joins the MB and/or ML on its path to the apical foramen.15 Most of the MM canals in the current study are confluent (87.5%), similar to that found by Azim, et al.,11 with 78.57% of MM canals being confluent and Nosrat, et al.,12 with a percentage equal to 46.7%. Both studies used operating microscope in all procedures.
Our study showed no difference in the MM canals considering the patient age; however, Nosrat, et al.,12 found a lower prevalence with increasing age, and Akbarzadeh, et al.,10 found a 4 times higher probability in patients under 42 years old. These studies used an operating microscope and a cone beam computed tomography, respectively. We attribute the difference in results due to the difficulty of locating of an MM canal without using an operating microscope, since in the present study this use occurred during the past 4 years only, probably reducing the number of MM canals analyzed.
In addition to magnification, surgical microscopy provides better illumination, which allows better differentiation of pulp chamber details.25,26 The microscope can improve the identification of extra canals in the mesial root, and this ability to locate MM canals in mandibular molars by 27x corroborates previous studies that reported increases of 16% to 20%.12,26 The prevalence of MM canals in the current study (2.9%) differs from other studies, probably because we used the operating microscope in only 35.63% of the cases, whereas the other studies used tomography,10 microtomography,17 and operating microscopy11 in all cases.
Conclusion
Extra canals in mandibular molars are more common in distal roots, first molars, and younger patients (<40 years old). Furthermore, extra roots are uncommon in mandibular molars in a Brazilian population. The relationship between extra canals or extra roots and patient gender was not statistically significant — a finding corroborated by other studies.9,12 It was troubling that there was no difference between the two treatment types, suggesting that, in most cases, extra canals are not found in the first treatment and, therefore, may require another intervention. Finally, this study reaffirms the importance of techniques that improve the quality of endodontic diagnosis such as using an operating microscopy and improving operators training and experience.
Acknowledgments
The authors would like to acknowledge the valuable contribution of the EndoMais Clinic for allowing them to complete the research.
When finding extra canals and roots, it’s important to make sure that all the roots are thoroughly cleaned. Read what Dr. Randy Garland has to say about complex root anatomy and apical periodontitis in “Healing of apical periodontitis in a maxillary second molar with fused roots and complex isthmus using the GentleWave® Procedure” here: https://endopracticeus.com/healing-of-apical-periodontitis-in-a-maxillary-second-molar-with-fused-roots-and-complex-isthmus-using-the-gentlewave-procedure/
- Tabassum S, Khan FR. Failure of endodontic treatment: The usual suspects. Eur J Dent. 2016;10(1):144-147.
- Vertucci FJ. Root canal anatomy of the human permanent teeth. Oral Surg. 1984;58(5):589-599.
- Wolf TG, Paqué F, Zeller M, Willershausen B, Briseño-Marroquín B. Root canal morphology and configuration of 118 mandibular first molars by means of micro-computed tomography: an ex vivo study. J Endod. 2016;42(4):610-614.
- Tomaszewska IM, Skinningsrud B, Jarzebska A, et al. Internal and external morphology of mandibular molars: an original micro-CT study and meta-analysis with review of implications in endodontic therapy. Clin Anat. 2018;31(6):797-811.
- Marceliano-Alves MF, Lima CO, Bastos, LGPMN, et al. Mandibular mesial root canal morphology using micro-computed tomography in a Brazilian population. Aust Endod J. 2019;45(1):51-56.
- Martins JNR, Gu Y, Marques D, Francisco H, Caramês J. Differences on the Root and Root Canal Morphologies between Asian and White Ethnic Groups Analyzed by Cone-beam Computed Tomography. J Endod. 2018;44(7):1096-104.
- Ferraz JA, Pécora JD. Three-rooted mandibular molars in patients of Mongolian, Caucasian, and Negro origin. Braz Dent J. 1993;3(2):113-117.
- Song JS, Choi HJ, Jung IY, Jung HS, Kim SO. The prevalence and morphologic classification of distolingual roots in the mandibular molars in a Korean population. J Endod. 2010;36(4) 653-657.
- Tahmasbi M, Jalali P, Nair MK, Barghan S, Nair UP. Prevalence of middle mesial canals and isthmi in the mesial root of mandibular molars: an in vivo cone-beam computed tomographic study. J Endod. 2017;43(7):1080-1083.
- Akbarzadeh N, Aminoshariae A, Khalighinejad N, et al. The association between the anatomic landmarks of the pulp chamber floor and the prevalence of middle mesial canal in mandibular first molars: an in vivo analysis. J Endod. 2017;43(11):1797-1801.
- Azim AA, Deutsch AS, Solomon CS. Prevalence of middle mesial canals in mandibular molars after guided troughing under high magnification: an in vivo investigation. J Endod. 2015;41(2):164-168.
- Nosrat A, Deschenes RJ, Tordik PA, Hicks ML, Fouad AF. Middle mesial canals in mandibular molars: incidence and related factors. J Endod. 2015;41(1):28-32.
- Kim KR, Song JS, Kim SO, et al. Morphological changes in the crown of mandibular molars with an additional distolingual root. Arch Oral Biol. 2013;58(3):248-253.
- Gu Y, Lu Q, Wang H, et al. Root canal morphology of permanent three-rooted mandibular first molars – part I: pulp floor and root canal system. J Endod. 2010;36(6):990-994.
- Pomeranz HH, Eidelman DL, Goldberg MG. Treatment considerations of the middle mesial canal of mandibular first and second molars. J Endod. 1981;7(12):565-568.
- Rodrigues CT, Oliveira-Santos C, Bernardineli N, et al. Prevalence and morphometric analysis of three-rooted mandibular first molars in a Brazilian subpopulation. J Appl Oral Sci. 2016;24(5):535-542.
- Versiani MA, Ordinola-Zapata R, Keles A, Alcin H, Bramante CM, Pécora JD, et al. Middle mesial canals in mandibular first molars: a micro-CT study in different populations. Arch Oral Bio. 2016;61:130-137.
- Silva EJ, Nejaim Y, Silva AV, Haiter-Neto F, Cohenca N. Evaluation of root canal configuration of mandibular molars in a Brazilian population by using cone-beam computed tomography: an in vivo study. J Endod. 2013;39(7):849-852.
- Caputo BV, Noro Filho GA, de Andrade Salgado DM, et al. Evaluation of the root canal morphology of molars by using cone-beam computed tomography in a Brazilian population: part I. J Endod. 2016;42(11):1604-1607.
- Estrela C, Bueno MR, Couto GS, et al. Study of Root Canal Anatomy in human permanent teeth in a subpopulation of Brazil’s center region using cone-beam computed tomography — part I. Braz Den J. 2015;26(5):530-536.
- Carvalho TS, Lussi A. Age-related morphological, histological and functional changes in teeth. J Oral Rehab. 2017;44(4):291-298.
- De Moor RJG, Deroose CAJG, Calberson FLG, The radix entomolaris and paramolaris: clinical approach in endodontics. J Endod. 2007;33(1):58-63.
- Carlsen O, Alexandersen V. Radix entomolaris: identification and morphology. Scand J Dent Res. 1990;98(5):363-373.
- Carlsen O, Alexandersen V. Radix paramolaris in permanent mandibular molars: identification and morphology. Scand J Dent Res. 1991;99(3):189-195.
- de Toubes KM, Côrtes MI, Valadares MA, et al. Comparative analysis of accessory mesial canal identification in mandibular first molars by using four different diagnostic methods. J Endod. 2012;38(4):436-441.
- Karapinar-Kazandag M, Basrani BR, Friedman S. The operating microscope enhances detection and negotiation of accessory mesial canals in mandibular molars. J Endod. 2010;36(8):1289-1294.
Stay Relevant With Endodontic Practice US
Join our email list for CE courses and webinars, articles and more..
