Dr. Chafic Safi says that preserving tooth structure with minimally invasive endodontics is easily achievable with the XP-3D™ Shaper and Finisher.

Dr. Chafic Safi discusses preserving as much healthy tooth structure as possible
It has been almost 100 years since 1925, when Walter Hess discovered the extensive and intricate nature of root canal anatomy. From that moment, the focus has always been on how to effectively clean, disinfect, and seal the root canal system. This has fueled multiple developments and technological advancements, making way for fascinating concepts and treatment philosophies, especially in the recent decade. Perhaps, the most spoken about recent development is minimally invasive endodontics (MIE).
What does “minimally invasive endodontics” mean?
To understand MIE, one has to understand minimally invasive dentistry. Minimally invasive dentistry can be defined as the preservation of healthy dental structure by preventing disease from occurring, intercepting its progress, but also removing and replacing with as little tissue loss as possible. In other words, the objective is minimal intervention.1
MIE is a technique that aims first and foremost at maintaining the vitality of the pulp. Should this vitality not be maintainable and root canal treatment indicated, healthy coronal, cervical, and radicular tooth structure should be preserved as much as possible.2 From treatment selection — root canal treatment versus vital pulp therapy to access opening, root canal cleaning and shaping, and obturation — the preservation of maximal dentin mass is of utmost importance.
With this objective in mind and in the context of biomechanical instrumentation, cleaning the canals while respecting their natural morphology is one of the minimally invasive approaches that can preserve radicular tissue. Recently, newly developed technologies and materials have emerged that allow minimally invasive endodontic procedures during instrumentation.
Root canal instrumentation, the traditional way
The primary goal of endodontic treatment is to access, shape, clean, and fill the complicated anatomy while leaving the tooth strong enough in order to maintain function. Today, many file systems with different taper and cutting efficiencies are available. These instruments cause varying levels of removed dentin volume and surface area in the root canals. During mechanical preparation, removing excessive amounts of dentin tissue or leaving behind uninstrumented areas cause failure. Thus, the target is to allow effective disinfection by being faithful to the original root canal anatomy and reaching an apical enlargement sufficient enough to achieve strong antimicrobial efficacy.

Traditional endodontic files cannot enlarge the natural cross section of the root in all directions; rather they induce a round shape, leaving large areas untouched and packing debris in the oval extremities.3 This prevents adequate cleaning and disinfection (Figure 1). Moreover, the more a canal is tapered with traditional instruments, the thinner and the weaker the tooth becomes. Traditional rotary instruments have consistently been shown to create dentinal defects and cracks that are suspected to lead to root fractures.4 Even reciprocating techniques create dentinal cracks, without mentioning their debris extrusion into the periapical tissues.5,6
This new XP-3D Shaper+ with the combination of the XP-3D Finisher, offer the clinician an easy, safe, and minimally invasive approach at performing root canal treatments as well as non-surgical retreatments.
Root canal instrumentation, the minimally invasive way
There are three important facts to remember:
- Traditional NiTi instrumentation techniques are deficient.
- Bacteria organize themselves as biofilm that is more difficult to remove than planktonic bacteria.
- Teeth are weakened by conventional instrumentation.
In order to address these shortcomings, a paradigm shift was needed whereby we move from the school of thought of the file shaping the canal to the canal shaping the file. In 2016, two unique instruments were launched with the promise of anatomical shaping and deep disinfection: the XP-3D™ Shaper and the XP-3D™ Finisher. These instruments were made using a newly patented NiTi alloy called MaxWire (Brasseler USA, Savannah, Georgia) with the special ability to change molecular structure, from the martensitic phase at room temperature to the austenitic phase at body temperature, allowing them to expand and adapt to the root canal wall in all directions and enhance irrigation. Both instruments when rotated at speeds of 800-1000 rpm would engage in a wider envelope of motion, creating a cleaner canal while conserving its original shape — minimally invasive anatomical instrumentation.
This year, the XP-3D Shaper got a new upgrade. It now comes in the austenitic phase regardless of temperature, making it more effective at cutting dentin while still offering the biological properties of anatomical shaping. This new XP-3D Shaper+ with the combination of the XP-3D Finisher, offer the clinician an easy, safe, and minimally invasive approach at performing root canal treatments as well as non-surgical retreatments.
So, what is this XP-3D Shaper+, and how does it work?
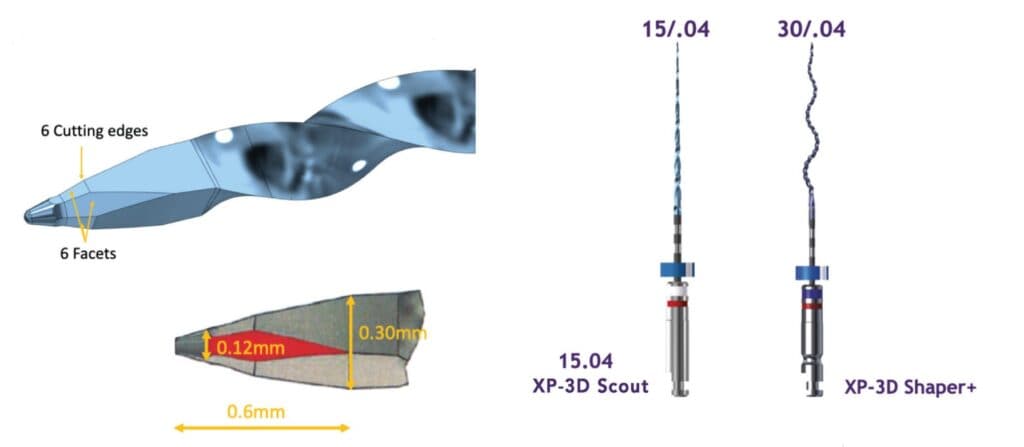
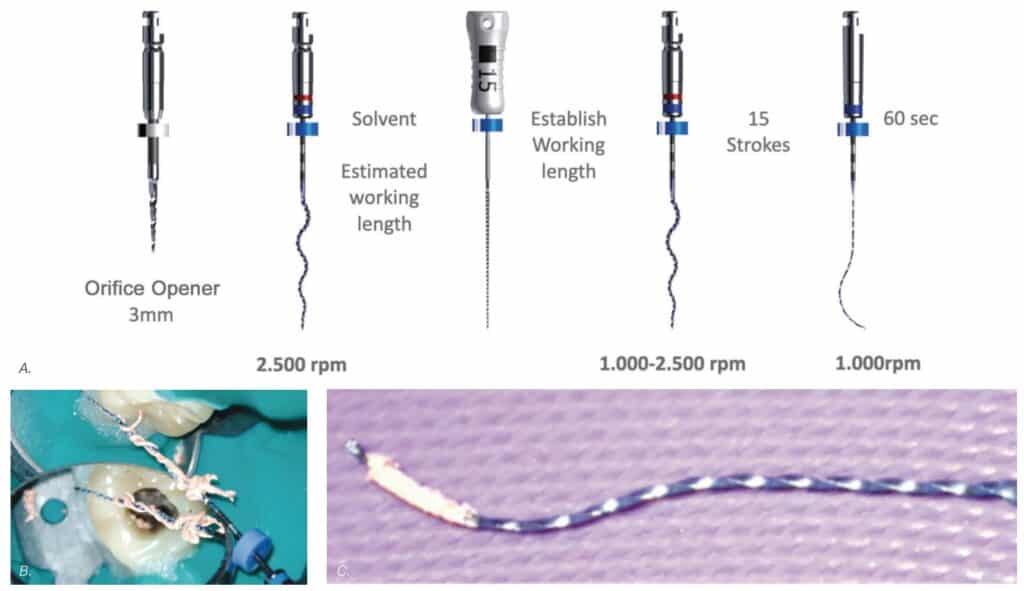
Just like its predecessor, The XP-3D Shaper+ features a small flexible core (#30/.01) that is extremely resistant to cyclic fatigue. The unique serpentine design allows the instrument to gently abrade the inner walls of the root canal, keeping the debris in suspension while the MaxWire® alloy allows its adaptation to the canal morphology without the stress associated with conventional NiTi file. With an initial taper of 1%, the XP-3D Shaper+ expands inside the canal to achieve a taper of 4%. Another cutting-edge technology included in the XP-3D Shaper+ is the tip which has a unique geometry. It comes with the Booster Tip made of six cutting edges aligned with six facets — versus three for the conventional XP-3D Shaper. This tip enables the instruments to start cleaning and cutting dentin at 0.6 mm from the tip with an initial cutting diameter of 0.12 mm, ensuring 0.30 mm diameter is reached at 0.6 mm from the tip (Figure 2). A glide path of at least 15.04 is required, which will be gradually increased to achieve 30.04. This design makes treatment shorter and easier to perform, reducing the risk of errors and incidents while preserving the natural shape of the canal. The XP-3D Shaper+ is employed at a speed of 1000 rpm and 1Ncm torque and can be used up to eight canals according to the following protocol: once working length is confirmed, a glide path up to size 15.04 is recommended. This is easily achievable with the XP-3D Scout (Brasseler USA, Savannah, Georgia) 15.04 file. Following that, the XP-3D Shaper+ can be used giving 2-5 strokes until working length is reached. The canal is then flushed with NaOCl or another irrigation solution like Triton® (Brasseler USA, Savannah, Georgia) and the XP-3D Shaper+ reintroduced with eight full strokes to working length, at which point the canal would have been anatomically cleaned and instrumented to a size 30.04.7 The advantage of using the aforementioned 15.04 file is that it functions at the same speed and torque as the XP-3D Shaper+, hence streamlining the procedure (Figure 3). This new instrument offers clinicians the possibility of letting the canal shape the file and solves two of the previously mentioned challenges: the deficiency of traditional NiTi instruments and their weakening of the dental structure.
Additionally, the XP-3D Shaper+ can also be used in retreatments. Thanks to its shape, it acts like a corkscrew engaging itself around gutta percha and pulling it out in large pieces (Figure 4). This way, there is no burnishing of the material against the root canal. A speed of 2500 rpm is required in order for the XP-3D Shaper+ to pull out the gutta percha. The XP-3D Shaper+ has been shown to remove gutta percha twice as fast as conventional files.8
What about the XP-3D Finisher?
The XP-3D Finisher file (Brasseler USA, Savannah, Georgia) has been designed with the aim of contacting areas in the longer aspect of the canal, where any conventional round file cannot reach. It is made using the MaxWire alloy which allows shifts in conformation from the martensite soft phase to the austenite robust phase, yielding a sickle/spoon shape at its tip. Additionally the XP-3D Finisher has no taper, making it extremely flexible and resistant to cyclic fatigue, so it does not enlarge the canal. When the tip is squeezed, the bulb can be expanded to 6 mm; and when the bulb is compressed, the tip will expand to 6 mm. The expansion of the bulb and tip act like a periodontal scaler but within the root canal, hence scraping and dislodging all the debris attached to the root canal walls, namely biofilm and stubborn gutta-percha tags in cases of retreatment. It is more effective than passive ultrasonic irrigation in reducing biofilm and the remaining root canal filling.9,10 This instrument comes in two tip sizes, a No. 25 and a No. 30. The No. 30 is also known as the Finisher-R, indicating its usefulness in retreatments. The No. 30 is slightly stiffer than the No. 25, making it an ideal wire to whip and detach stubborn gutta percha.
Finally, the XP-3D Finisher causes turbulence of the irrigant, maximizing the anti-microbial effect and therefore achieving deep disinfection in a safe and anatomical fashion.
Once inside the canal, the XP-3D Finisher is rotated for 60 seconds at 1000 rpm, moving it up and down at an amplitude of 7 mm to 8 mm in order to adequately spread the action of the tip and the bulb. The canal has to be filled with NaOCl or Triton and should be minimally prepared to a size ISO25 for the No. 25 Finisher and to a size ISO30 for the No. 30 Finisher.
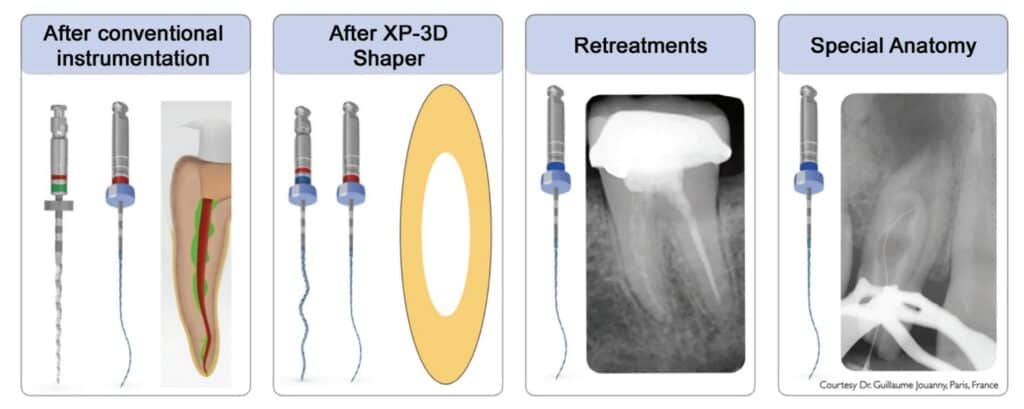
The XP-3D Finisher is indicated to be used (Figure 5):
- After conventional NiTi instrumentation
- After XP-3D Shaper+ especially in oval canals
- In retreatment cases
- In special anatomical cases such as internal resorptions, dens in dente, and immature roots
With the XP-3D Finisher in a clinician’s armamentarium, eliminating biofilm and maximizing disinfection is now possible in a minimally invasive fashion.
Where do we go from here?
Minimally invasive instrumentation during root canal treatment aims at exerting microbial control while preserving tooth structure and supporting tissues, especially coronal and radicular dentin. Many instruments varying in flexibility and metallurgical properties have been produced in the past, however none have been able to clean the root canal system anatomically. Today, the combination of two instruments, the XP-3D Shaper+ and the XP-3D Finisher, offer the possibility to debride, clean, and disinfect, while adapting to the canal’s natural anatomy in a simple, safe, efficient, and conservative fashion. All of these factors make minimally invasive endodontic treatment more possible and successful.
- Ericson D. What is minimally invasive dentistry? Oral Health Prev Dent. 2004;2 Suppl 1:287-292.
- Gluskin AH, Peters CI, Peters OA. Minimally invasive endodontics: challenging prevailing paradigms. Br Dent J. 2014 Mar;216(6):347-353.
- Paqué F, Balmer M, Attin T, Peters OA. Preparation of oval-shaped root canals in mandibular molars using nickel-titanium rotary instruments: a micro-computed tomography study. J Endod. 2010 Apr;36(4):703-707.
- Shemesh H, Bier CA, Wu MK, Tanomaru-Filho M, Wesselink PR. The effects of canal preparation and filling on the incidence of dentinal defects. Int Endod J. 2009 Mar;42(3):208-213.
- Elayouti A, Chu AL, Kimionis I, Klein C, Weiger R, Löst C. Efficacy of rotary instruments with greater taper in preparing oval root canals. Int Endod J. 2008 Dec;41(12): 1088-1092.
- Caviedes-Bucheli J, Castellanos F, Vasquez N, Ulate E, Munoz HR. The influence of two reciprocating single-file and two rotary-file systems on the apical extrusion of debris and its biological relationship with symptomatic apical periodontitis. A systematic review and meta-analysis. Int Endod J. 2016 Mar;49(3):255-270. Epub 2015 Apr 22.
- Azim AA, Piasecki L, da Silva Neto UX, Cruz ATG, Azim KA. XP Shaper, A Novel Adaptive Core Rotary Instrument: Micro-computed Tomographic Analysis of Its Shaping Abilities. J Endod. 2017 Sep;43(9):1532-1538.
- Azim AA, Wang HH, Tarrosh M, Azim KA, Piasecki L. Comparison between Single-file Rotary Systems: Part 1-Efficiency, Effectiveness, and Adverse Effects in Endodontic Retreatment. J Endod. 2018 Nov;44(11):1720-1724.
- Bao P, Shen Y, Lin J, Haapasalo M. In Vitro Efficacy of XP-endo Finisher with 2 Different Protocols on Biofilm Removal from Apical Root Canals. J Endod. 2017 Feb;43(2):321-325.
- Alves FR, Marceliano-Alves MF, Sousa JC, Silveira SB, Provenzano JC, Siqueira JF Jr. Removal of Root Canal Fillings in Curved Canals Using Either Reciprocating Single- or Rotary Multi-instrument Systems and a Supplementary Step with the XP-Endo Finisher. J Endod. 2016 Jul;42(7):1114-1119.
Stay Relevant With Endodontic Practice US
Join our email list for CE courses and webinars, articles and more..
