For part 3 of his series, Dr. Nishan Odabashian discusses treatment of teeth with failing previous root canal treatment exhibiting large radiolucencies
Introduction
A healthy 30-year-old female presented to our office on December 13, 2012, after her mother, a previous patient, insisted that she obtain a second opinion prior to having her tooth in the left mandibular molar area extracted as she was advised by her general dentist. She was referred to an oral surgeon for an extraction, bone graft, and implant with an implant-supported crown as the final restoration.
[userloggedin]
Clinical findings and dental history
The patient had a crown on tooth No. 19, which according to the patient, was placed 5 years prior. She had composite and amalgam restorations on her remaining maxillary and mandibular premolar and molar teeth in the quadrant. The patient did not have any intraoral swelling but had been experiencing dull pain on the tooth for some time. However, she had been too busy to have the problem evaluated earlier. Both teeth No. 18 and No. 20 responded normally to cold sensitivity testing. Probing depths were within normal limits, measuring 2 mm-3 mm as probed at eight different sites around the tooth, using the “walking-the-probe technique.”
Radiographic findings
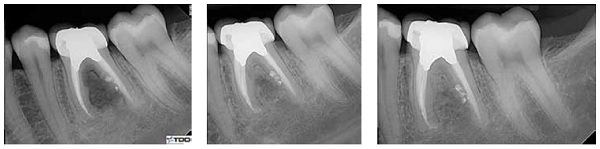
Periapical and bitewing radiographs pointed to a large “unilocular” lucency in the furcation area of tooth No. 19. The lucency extended almost the entire length of the roots from the furcal aspect. Tooth No. 19 had a previous root canal treatment that the patient noted had taken place approximately 10 years prior. The tooth had a screw-type post in the distal root, a core, and a PFM crown, with the apical resorption apparent in the mesial apex and mesial aspect of the distal root.
Medical history
Medical history was non-contributory.
Diagnosis
- Pulpal: Pulpless — Previously treated root canal
- Periapical: Symptomatic peri-radicular periodontitis
Differential diagnosis
- Lesion of endodontic origin
- PA cyst
- PA granuloma
- Other
Treatment plan options
- Initiate retreatment, and based on short-term response, determine proximate course of action — i.e., continue retreatment protocol or send for extraction/implant.
- Refer for extraction.
Treatment
The patient wanted to think about her treatment options and advise us of her decision. Six weeks after the initial consultation, the patient finally decided that she would give retreatment a try.


Retreatment was initiated by isolating with a rubber dam and accessing the crown, removing the core and the screw post from the distal canal, as well as removing gutta percha from all canals. It could be seen that there was a viscous material resembling pus in close contact to the apical gutta percha. The canals and pulp chamber were flushed with copious amounts of sodium hypo-chlorite. During drying of the canals, dark material adhered to the paper points. The canals were then irrigated, dried, and dressed with calcium hydroxide. The tooth was temporized with Cavit™. The patient was seen again during the 2 following weeks to continue cleaning the canals of their contents, again remedicated with calcium hydroxide for 10 weeks, and again 6 weeks later.


The patient presented for her next appointment almost 4 months after initiation of retreatment; there was a slight improvement of the furcal lucency. However, it was less than what was expected. At this appointment, after further cleaning, MTA was placed in the distal canal to seal the perforation on the mesial aspect of the distal root. The patient was seen at 6 weeks and 3 months after to monitor the healing and osseous repair.


We were able to notice clear ossous regeneration in the furcation area at the next visit, which was 8 months after the initiation of the retreatment process. Calcium hydroxide was again placed in the mesial canals for 3 more months, and completion of the treatment was planned for the next visit.
It was now 1 year since the initiation of the retreatment. The healing of the furcal bone was phenomenal. Both the operator and the patient were very pleased with the results. The mesial roots were obturated with gutta percha, and an amalgam core buildup was placed.
One year after the initiation of the retreatment, the patient presented for the obturation appointment. The healing and regeneration of the furcal bone were phenomenal. Both operator and patient were very pleased with the results.
Follow-up
Follow-ups continued every 3 months for the first year, and for 6 months during the second year after the completion of the procedure. At the 2-year follow-up, one can see an almost complete resolution of the furcation lucency. This was accomplished without any surgery and without any grafts. The patient is completely asymptomatic and is able to use the tooth in full function.
Discussion
This case presentation is a third in a series of teeth exhibiting large periradicular lucencies associated with failing root canal treatments. (The first two articles were published in Endodontic Practice US in May/June 2014, Vol. 7 No. 3 and January/February 2015, Vol. 8 No. 1.) As mentioned in the two previous reports, treatment of teeth with large lucencies requires more than the garden-variety retreatment or surgery. It requires time, patience, proper follow-up, sound restorative treatment, proper diagnosis and, when needed, involvement of other specialists.
Treatment of teeth with large lucencies requires more than the garden-variety retreatment or surgery.
In this case, the 30-year-old female patient was slated to go through an extraction and extensive bone and soft tissue grafting surgery with the loss of her tooth. And although neither the general dentist nor the oral surgeon can be faulted for the treatment that was about to be rendered, publication of these types of treatment results allow for the consideration of the possibility of retaining these teeth with long-term endodontic treatment.
The titrated-type of treatment which was rendered allowed us to “throw in the towel” if the signs and symptoms had not improved. At such time, the option of extraction, grafting, and implant placement would be performed. By attempting to treat the lucency and save the tooth, the implant option is never taken “off the table.”
This case also shows the capacity of the body to heal if and when the offending insults are removed. It shows the result of patience and taking the time to perform the most conservative dental treatment possible. It would have been easier (for the endodontist) to “just extract” and after surgery and grafting, to place an implant and implant-supported crown. It was definitely more time-consuming for this clinician, but also much more rewarding. The treatment rendered was much less invasive, much less expensive, and was associated with less morbidity for the patient.


Summary
This case shows what is possible with endodontic treatment/retreatment as far as osseous healing of large periradicular lucencies. This case also shows the benefit of multi-visit endodontic retreatment. Titrated treatment is very useful in these types of cases. It allows for re-evaluation of the results (or lack thereof) during the course of treatment.
Stay Relevant With Endodontic Practice US
Join our email list for CE courses and webinars, articles and more..
