Bleeding during implant surgery can be a stressful complication. Drs. Lanka Mahesh, Gregori M. Kurtzman, Sagarika Shukla, and Zara Dhawan share how to avoid this obstacle.
Drs. Lanka Mahesh, Gregori M. Kurtzman, Sagarika Shukla, and Zara Dhawan discuss management of a surgical complication
Abstract
Implant placement for missing teeth has become a routine procedure to establish the functional and esthetic needs of the patient. And just like any surgical procedure, complications like bleeding, infection, etc., can occur during implant placement as well. Bleeding from the alveolar antral artery (AAA) is one such complication which causes bleeding, and any clinician should be prepared for its management. Authors will discuss one such case and the management of this complication. CBCT is a very important diagnostic tool which should be used for every case possible.
Introduction
Implant placement has become a common procedure when one has to rehabilitate missing teeth functionally and esthetically. With better understanding and advances in technology, many procedures are available to rehabilitate the maxillary arch, and clinicians have many options of bypassing the sinus such as zygoma implants, the All-on-4 technique, indirect sinus lifts or graftless solutions, and short implants. However, each aforementioned technique is not as predictable as a direct sinus lift, especially in cases of a severely atrophic maxilla.1,2 Short implants have less bone-to-implant contact and have more chances of failure in load-bearing areas. In a meta-analysis by Papaspyridakos, et al.,3 authors stated that short implants (≤6 mm) have less predictable survival rates compared to longer implants (>6 mm) after periods of 1-5 years in function. When it comes to an indirect sinus lift, the procedure does not increase the height of maxillary sinus sufficiently,4 leaving a direct sinus lift a predictable treatment choice. However, many patients are anxious about maxillary sinus grafting and the complications which follow the surgery, hence procedures like All-on-4 were developed which can rehabilitate the entire arch along with bypassing the sinus.
In this type of clinical situation, knowledge of anatomy and the arterial blood supply becomes paramount. Structure wise, the maxillary sinus (MS) is pyramidal in shape and largest of the paranasal sinuses.5 The anterior wall of the MS is formed by the facial surface of the maxilla and is internally grooved by the canalis sinuosus (which houses the anterior superior alveolar nerve and vessels).5 It receives blood supply via the maxillary artery and its branches. In this article, the artery of interest is alveolar antral artery (AAA), which is an anastomosis of the posterior superior alveolar artery (PSAA) and the infraorbital artery (IOA).6 As the name suggests, it appears on the maxillary facial plate near to or in close approximation with maxillary second premolar and first molar area, a position from where it takes a U-turn, roughly paralleling the sinus floor. Not much has been reported regarding this artery in the literature as it goes undetected, and the clinician only comes to know when it interferes during osteotomy (10%-30% of cases) or any complication.7,8 It has higher detection rates in males due to larger diameters, as well as in narrower maxillary sinuses <14 mm in width. The immediate complication is bleeding, which can be called as the “gateway complication” further leading to a series of complications that impact treatment prognosis and outcome and or abortion of the surgical procedure.6,9
The vertical distance of the artery from the alveolar ridge varies in patients depending upon the resorption of the ridge. Solar, et al.,10 reported a range of 15 mm – 25 mm of vertical positioning of the artery in alveolar bone in a mixed dentate/edentulous population. However, a more reliable measurement, which had been found to be mean of 7.66 mm, could be found via CBCT, where ridge resorption would not influence the vertical distance.11 Park, et al.,12 found this height to be between 7.71 mm – 8.01 mm, and suggested a lateral window of 8 mm for visualization, instrumentation, and graft placement if the sinus lift is to be performed. Studies have shown that the artery has an average diameter of 1.5 mm,13 and that a diameter of < 0.5 mm does not indicate any significant bleeding that would interfere with surgery.14 However, Testori, et al.,15 suggested that a small caliber vessel on CBCT, may correspond to a much larger caliber vessel clinically.
Case report
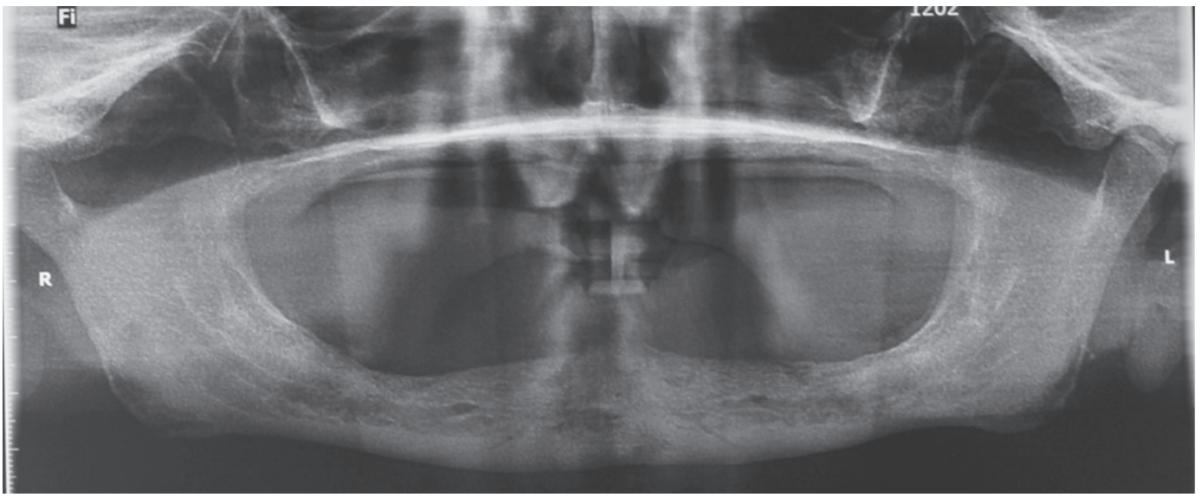
A 59-year-old male reported to the dental office with missing maxillary teeth due to poor oral hygiene. Treatment planning was done for all on four implant placements followed by prosthesis. A complete medical history was obtained and was negative for any significant medical problems. The patient denied being allergic to any medication as well. The patient agreed to the implant placement and was advised to have an orthopantomogram (Figure 1).

On the day of the surgery, before commencing the procedure under strict asepsis, the patient was asked to rinse with 0.12% chlorhexidine gluconate mouthwash (Peridex™; 3M™). Local anesthesia with a vasoconstrictor was infiltrated buccally and palatally into the posterior and anterior maxilla on both the sides using S-blades (straight) (Zabby, India). The incision was made on the crest of the ridge in the region of teeth Nos. 15-25. While creating the incision, bleeding was noticed in the region of tooth No. 15 which intensified during the flap reflection (Figure 2). Bleeding was pulsatile, indicating an arterial bleed. Initially attempts to control bleeding included a pressure pack and ice pack, and the bleeder was isolated, and the vessel ligated (Figure 3). The bleeding could be controlled, and the procedure was completed by placing four Bioner implants (Bioner, Spain), size 4/10 mm. Sutures were placed, and patient was kept on basic medication for pain and infection control. Immediately after the surgery, the patient was advised to get a CBCT. As shown in Figure 4, a coronal view and Figure 4B (yellow arrows), the position of the artery can be seen.
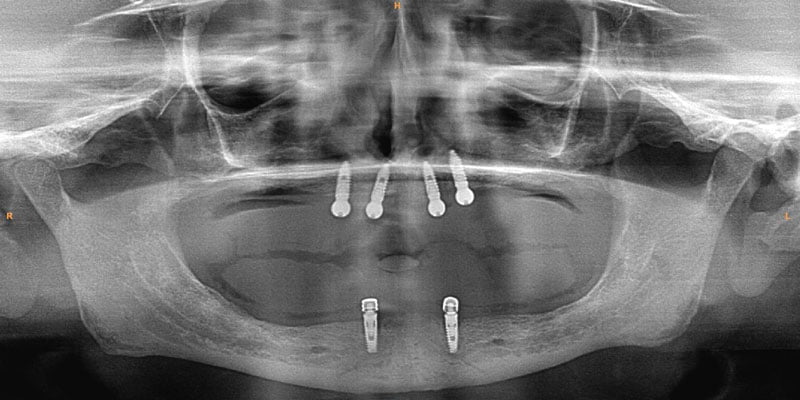
In the follow-up sessions, the patient was comfortable, but did complain of mild swelling which subsided within 4-5 days. A post-op CBCT showed excellent recovery, bone width, and proper implant placement (Figure 5).
Discussion
Encountering a, AAA complication during an All-on-4 procedure in the region of teeth Nos. 14 and 15 has not been reported so far, however literature reports bleeding complications from AAA during sinus-lift procedures. Another complication that occurs is infection in about 3% of the cases, and in 1% of the cases loss of graft,16 and this usually happens after hematoma formation. In simple terms, the larger the vessels, the more the bleeding will occur. According to Ella, et al.,17 the risk involving AAA in osteotomies can be >10%, whereas according to authors Chan and Wang18 and Elian, et al.,8 it is 20%. Authors Jensen, et al.,19 have reported severe bleeding in sinus elevation surgery through a transcrestal approach, wherein bleeding led to swelling and consecutive hospitalization for 3 days, after which, normal functioning was regained. Hence management of the complication plays an important part for the clinician.
The first and foremost solution is the application of pressure pack and ice pack to control the bleeding along with topical thrombin. Other products such as SURGICEL® Absorbable Hemostat, SURGICEL™ Powder (Surgicel; Johnson & Johnson Co., Somerville, New Jersey), and bone wax can also be used. Usually because of bleeding at the surgical sight, pinpointing the exact bleeding spot becomes difficult, but if that can be isolated, then electrocautery/chemocautery or ligation can be done. As aforementioned, if the vessel is large, and bleeding cannot be controlled, the procedure should be aborted, and patient should be hospitalized.
Use of piezoelectric devices safely bypasses the vessels as it only cuts the bony surface, avoiding any chance of vessel rupture. The only disadvantage is that it is a time-consuming method, but better when it comes to any complication or aborting the procedure. In a surgical double-window technique described by Maridati, et al.,20 an osteotomy is made above and below the vessel, leaving a thin bridge of bone holding the vessel intact. However, this is a difficult technique to follow and does not work in terms of instrumentation, implant placement, and septated sinuses.6 The simplest of the methods to avoid this complication is detection which is best achieved with CBCT, however even with CBCT, AAA can be detected in only 50% of the cases,22 perhaps because the vessel is too small to be detected by CBCT, which does not mean that there is an absent vessel, or anastomosis does not exist. Cadaveric studies have shown that anastomosis is present 100% of the time,23 but it goes undetected or unreported, simply because many clinicians assume that the anastomosis does not exist or use basic radiographic techniques for the implant placement.
In the case discussed here, authors encountered a small vessel wherein the bleeding was easily controlled with pressure packs and ice packs. The site of implant placement is a safe zone, and such a bleeding complication usually occurs during sinus-lift procedures and not in the anterior region. A simple detection could have helped clinicians to plan osteotomy better. Fortunately, the vessel was not big, and the bleeding could be controlled by ligation. Otherwise the implant placement may have had to be postponed. This proves that CBCT is an excellent tool and should be used more often for the case planning and detection of pathologies.21
Conclusion
Dental radiographs are an important tool in accurate diagnosis and treatment planning.21 Imaging is also the most common and important investigation carried out before any dental procedure that requires surgical or corrective intervention.21 Thus, accuracy of the X-ray, whether it is an intraoral periapical radiograph (IOPA) or an orthopantomogram (OPG) becomes paramount. However, these investigative tools provide a 2D image of a 3D object and are subject to false positive errors. Also, patients should be counselled and motivated to receive the proper imaging for the procedure. Above all, the surgeon must anticipate and effectively manage complications encountered during the surgery.
For more ways to mitigate bleeding during implant procedures, read Dr. Steven Vorholt’s article, “The importance of suturing in dental implant surgery,” at https://endopracticeus.com/ce-articles/the-importance-of-suturing-in-dental-implant-surgery/. Subscribers can take the quiz and receive 2 CE credits!
 Lanka Mahesh, BDS, MBA, completed a bachelor’s degree in dental surgery and a diploma in hospital administration and is currently pursuing a PhD in Integrated Implantology. He has published over 225 articles and authored several textbooks. He practices in a private specialized implant practice at The Specialist Clinic in New Delhi, India and can be reached at drlanka.mahesh@gmail.com.
Lanka Mahesh, BDS, MBA, completed a bachelor’s degree in dental surgery and a diploma in hospital administration and is currently pursuing a PhD in Integrated Implantology. He has published over 225 articles and authored several textbooks. He practices in a private specialized implant practice at The Specialist Clinic in New Delhi, India and can be reached at drlanka.mahesh@gmail.com.
 Gregori Kurtzman, DDS, is in private general dental practice in Silver Spring, Maryland. He is a former Assistant Clinical Professor at University of Maryland in the department of Restorative Dentistry and Endodontics and a former AAID Implant Maxi-Course assistant program director at Howard University College of Dentistry. He has lectured internationally on the topics of restorative dentistry, endodontics and implant surgery, removable and fixed prosthetics, and periodontics. He has over 870 published articles, as well as several ebooks and textbook chapters. He can be reached at dr_kurtzman@maryland-implants.com.
Gregori Kurtzman, DDS, is in private general dental practice in Silver Spring, Maryland. He is a former Assistant Clinical Professor at University of Maryland in the department of Restorative Dentistry and Endodontics and a former AAID Implant Maxi-Course assistant program director at Howard University College of Dentistry. He has lectured internationally on the topics of restorative dentistry, endodontics and implant surgery, removable and fixed prosthetics, and periodontics. He has over 870 published articles, as well as several ebooks and textbook chapters. He can be reached at dr_kurtzman@maryland-implants.com.
 Sagarika Shukla, MDS, has a degree in periodontics with a special interest in facial esthetics. She is in private practice at The Specialist Clinic in New Delhi, India.
Sagarika Shukla, MDS, has a degree in periodontics with a special interest in facial esthetics. She is in private practice at The Specialist Clinic in New Delhi, India.
 Zara Dhawan, BDS, is in private practice at The Specialist Clinic in New Delhi, India. She graduated from the School of Dental Sciences, Sharda University, Uttar Pradesh, India, in 2020.
Zara Dhawan, BDS, is in private practice at The Specialist Clinic in New Delhi, India. She graduated from the School of Dental Sciences, Sharda University, Uttar Pradesh, India, in 2020.
- Chipaila N, Marini R, Sfasciotti GL, Cielo A, Bonanome L, Monaco A. Graftless sinus augmentation technique with contextual placement of implants: a case report. J Med Case Rep. 2014 Dec 17;8:437.
- Bedrossian E, Rangert B, Stumpel L, Indresano T. Immediate function with the zygomatic implant: a graftless solution for the patient with mild to advanced atrophy of the maxilla. Int J Oral Maxillofac Implants. 2006 Nov-Dec;21(6):937-942.
- Papaspyridakos P, De Souza A, Vazouras K, Gholami H, Pagni S, Weber HP. Survival rates of short dental implants (≤6 mm) compared with implants longer than 6 mm in posterior jaw areas: A meta-analysis. Clin Oral Implants Res. 2018 Oct;29 Suppl 16:8-20.
- Balaji SM. Direct v/s Indirect sinus lift in maxillary dental implants. Ann Maxillofac Surg. 2013 Jul;3(2):148-153.
- Standring S., ed. Gray’s anatomy: the anatomical basis of clinical practice.41st ed. London: Elsevier Health Sciences; 2015.
- Yang D, Lee N. A Simple Method of Managing the Alveolar Antral Artery during Sinus Lift Surgery.Int J Otolaryngology Head Neck Surg. 2021;10(3):131-146.
- Lee CY. Brisk, prolonged pulsatile hemorrhage during the sinus graft procedure: a case report with discussion on intra-operative hemostatic management. Implant Dent. 2010 Jun;19(3):189-195.
- Elian N, Wallace S, Cho SC, Jalbout ZN, Froum S. Distribution of the maxillary artery as it relates to sinus floor augmentation. Int J Oral Maxillofac Implants. 2005 Sep-Oct; 20(5):784-787.
- Varela-Centelles P, Loira M, González-Mosquera A, Romero-Mendez A, Seoane J, García-Pola MJ, Seoane-Romero JM. Study of factors influencing preoperative detection of alveolar antral artery by CBCT in sinus floor elevation. Sci Rep. 2020 Jul 2;10(1):10820.
- Solar P, Geyerhofer U, Traxler H, Windisch A, Ulm C, Watzek G. Blood supply to the maxillary sinus relevant to sinus floor elevation procedures. Clin Oral Implants Res. 1999 Feb;10(1):34-44.
- Varela-Centelles P, Loira-Gago M, Gonzalez-Mosquera A, Seoane-Romero JM, Garcia-Martin JM, Seoane J. Distance of the alveolar antral artery from the alveolar crest. Related factors and surgical considerations in sinus floor elevation. Med Oral Patol Oral Cir Bucal. 2016 Nov 1;21(6):e758-e765.
- Park WH, Choi SY, Kim CS. Study on the position of the posterior superior alveolar artery in relation to the performance of the maxillary sinus bone graft procedure in a Korean population. J Korean Assoc Oral Maxillofac Surg. 2012;38(2):71-77.
- Kim JH, Ryu JS, Kim KD, Hwang SH, Moon HS. A radiographic study of the posterior superior alveolar artery. Implant Dent. 2011 Aug;20(4):306-310.
- Rysz M, Ciszek B, Rogowska M, Krajewski R. Arteries of the anterior wall of the maxilla in sinus lift surgery. Int J Oral Maxillofac Surg. 2014 Sep;43(9):1127-30.
- Testori T, Rosano G, Taschieri S, Del Fabbro M. Ligation of an unusually large vessel during maxillary sinus floor augmentation. A case report. Eur J Oral Implantol. 2010 Autumn;3(3):255-258.
- Chiapasco M, Casentini P, Zaniboni M. Bone augmentation procedures in implant dentistry. Int J Oral Maxillofac Implants. 2009;24 Suppl:237-259.
- Ella B, Sédarat C, Noble Rda C, Normand E, Lauverjat Y, Siberchicot F, Caix P, Zwetyenga N. Vascular connections of the lateral wall of the sinus: surgical effect in sinus augmentation. Int J Oral Maxillofac Implants. 2008 Nov-Dec;23(6):1047-1052.
- Chan HL, Wang HL. Sinus pathology and anatomy in relation to complications in lateral window sinus augmentation. Implant Dent. 2011 Dec;20(6):406-412.
- Jensen SS, Eriksen J, Schiodt M. Severe bleeding after sinus floor elevation using the transcrestal technique: a case report. Eur J Oral Implantol. 2012 Autumn;5(3):287-291.
- Maridati P, Stoffella E, Speroni S, Cicciu M, Maiorana C. Alveolar antral artery isolation during sinus lift procedure with the double window technique. Open Dent J. 2014 May 30;8:95-103.
- Shukla S, Chug A, Afrashtehfar KI. Role of Cone Beam Computed Tomography in Diagnosis and Treatment Planning in Dentistry: An Update. J Int Soc Prev Community Dent. 2017 Nov;7(Suppl 3):S125-S136.
- Ilgüy D, Ilgüy M, Dolekoglu S, Fisekcioglu E. Evaluation of the posterior superior alveolar artery and the maxillary sinus with CBCT. Braz Oral Res. 2013 Sep-Oct;27(5):431-437.
- Bernardi S, Mummolo S, Ciavarelli LM, Li Vigni M, Continenza MA, Marzo G. Cone beam computed tomography investigation of the antral artery anastomosis in a population of Central Italy. Folia Morphol (Warsz). 2016;75(2):149-153.
Stay Relevant With Endodontic Practice US
Join our email list for CE courses and webinars, articles and more..
