Jordan Reiss examines how implants can fit into the endodontic practice
It’s the specialty’s most challenging question that no one wants to answer: Should endodontists be placing implants? There’s a wide range of opinions; just by reading that sentence, you’re probably mentally shouting at the page for or against. Whatever your answer may be, we must face the question head-on by looking at the pros and cons, the facts and the myths, of endodontists placing implants. It’s a new year, and it’s the perfect time to examine how implants could affect your specialty, your practice, and your patients in 2017.
 Why implants? Why now?
Why implants? Why now?
The demand for implants has been steadily increasing for several reasons. First, an increased standard of living has made procedures that were once cost-prohibitive more accessible to more people. Also, the population is aging, yet living longer, and is seeking a solution that provides comfort and better esthetic results than dentures or bridges could. Finally, digital technology such as cone beam computed tomography (CBCT) and 3D imaging software makes placing implants, if not “easier,” certainly more predictable for doctors.
With demand on the rise, we’re finding there’s simply not enough supply — i.e., doctors who are specialized in planning and placing implants. Consider periodontists, who for years weren’t trained to place implants but are now doing implant surgeries and placements. In fact, today, nearly every specialty is placing implants in some capacity, even GPs.
The scope of endodontics
While the question of which specialty should place implants may be a contested topic, the path for endodontists to do so has been being quietly paved for years. In 2013, the American Association of Endodontists (AAE) Special Committee on the Scope of Endodontics published a position statement confirming that the “placing of dental implants is within the scope of practice of endodontics.”1 The AAE also clearly references implants in its joint position statement with the American Academy of Oral and Maxillofacial Radiography (AAOMR)2 on the use of CBCT. As Recommendation 10 states: “Limited field of view CBCT should be considered as the imaging modality of choice for surgical placement of implants.”
Education is key
In 2006, the Commission on Dental Accreditation (CODA) endodontic standards was revised to increase endodontists’ knowledge of placing endodontic endosseous implants from “familiarity” to “understanding.”1 This understanding can only be gained through specialized training — a must for any doctor before placing implants. In fact, today, some endodontic programs do teach implants. As further evidence that implant placement by endodontists is on the rise, from 2008-2011 there were 37 sessions at AAE continuing education events on dental implants,1 and in 2009, the AAE fall conference topic was “Implants and Endodontics, Treatment Planning and Placement Techniques.”1
Is placing implants right for you?
In 2009, a survey sent to 1,500 endodontists in the United States revealed that 57% supported the specialty placing implants.3 However, there are a few important qualifiers here. How will placing implants affect your referral relationships? Contact your referrals to see if they’d be comfortable referring patients to you. Endodontists who have been trained to place implants are more likely to be included in the treatment plan with their referring doctors. How will it affect your bottom line? Being able to offer an additional service to your patients could be a new source of revenue. Most important, by placing implants, are you providing the best care for your patients? Endodontists may be the least biased when it comes to the “who should place implants” debate, as their job is to save teeth; however, sometimes, an implant may be the only alternative. It can be discouraging for a patient (who’s already come from another doctor) to hear their endodontist say, “I’m sorry, there’s nothing I can do.” Therefore, the ability to place implants could be a relief to patients who wouldn’t have to be referred out to yet another specialist.
What’s next?
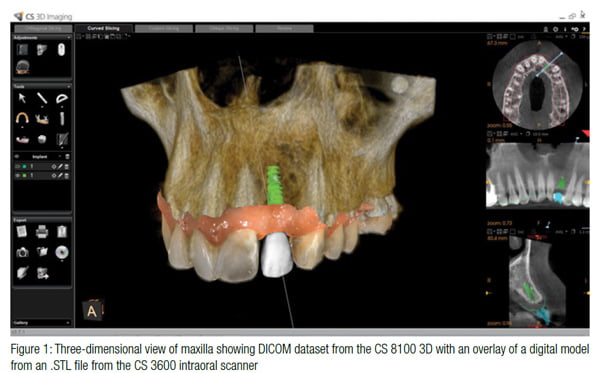
If you decide that placing implants is right for you, and assuming you have the appropriate knowledge and training, you’ll need the right tools. When it comes to placing implants today, it’s arguably the standard of practice that a CBCT scan should be taken. Fortunately, most modern endodontists already have experience with CBCT and know firsthand how a scan can aid in diagnosis. Often, the same small FOV, high-resolution low-dose scan — such as one captured by the CS 8100 3D system — taken to evaluate whether a tooth can be saved could also be used to evaluate challenging anatomical variability, pathology and bone quality, and quantity for placement of an implant.
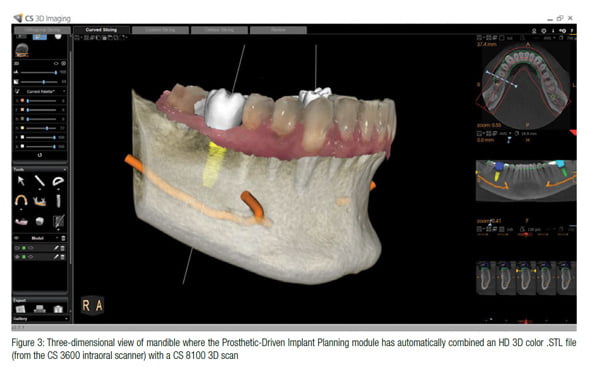 Also, Carestream Dental’s CS 3D Imaging software is one of many software platforms that include an implant library from the top implant manufacturers to streamline virtual implant planning. After virtual implant placement, the 3D image can be used for patient education or for more comprehensive analysis. Carestream Dental also provides a plethora of educational resources to clinicians for learning how to use the virtual implant function and implant library of its software.
Also, Carestream Dental’s CS 3D Imaging software is one of many software platforms that include an implant library from the top implant manufacturers to streamline virtual implant planning. After virtual implant placement, the 3D image can be used for patient education or for more comprehensive analysis. Carestream Dental also provides a plethora of educational resources to clinicians for learning how to use the virtual implant function and implant library of its software.
Only you can determine if placing implants is right for you, your practice, and your patients. However, having some level of knowledge of placing implants is crucially important for endodontists. If a tooth is unable to be saved, the patient who has come to you for your specialty knowledge is going to ask your opinion about next steps. Whether you plan to place implants or not, I sincerely hope you’ll learn more about the role of implants in the endodontic practice. Taking the time to learn more about implant placement may help your referrals, provide salient information to your patients, and ultimately, help you make the decision whether or not to place implants in your practice now or possibly in the future.
Stay Relevant With Endodontic Practice US
Join our email list for CE courses and webinars, articles and more..
