Dr. John West recognizes that the best education in the world is an endodontist’s own personal education
In 1966, British actor Michael Caine was an Oscar nominee for his movie Alfie, as was the Burt Bacharach and Hal David song of the same name that begins with the lyrics: What’s it all about, Alfie? Caine has appeared in more than 150 films, plays, and television shows, and he’s not done yet. Professor Dr. Herbert Schilder passed away 5 years ago in 2008. Had he lived, like Caine, he would not have been done. In fact, at age 80, like actor Michael Caine, he would have been at the top of his game.
Dr. Schilder always asked, “What’s it all about?” In his search for the answer, he did not discover the human root canal system, but he was the first to identify the relationship of root canal system anatomy, endodontic mechanics, and endodontic predictability. He changed the endodontic landscape. He changed the language of endodontics.1,2 Schilder also did not invent the root canal system, but he was the first to refer to the root canal as a “system” versus a simple tunnel. Schilder was the first to popularize sodium hypochlorite for cleaning away “dentin mud” (dentin filings packed inadvertently into the apical zone) and digesting detached dental pulp. In fact, Schilder used to call dentin mud the “fatal flaw” of endodontics. It still is today. When I was in my third year of dental school, sodium hypochlorite was not protocol. Instead, alcohol was the preferred endodontic irrigant but did not affect detached pulp, biofilm, or necrotic pulp. Next, Schilder suggested calling oramina portals of exit (POEs). A portal of exit could be a foramen, an iatrogenic perforation, or a resorptive perforation. All root canal system communications with the attachment apparatus are communications nonetheless, requiring a hermetic seal in order to make endodontic treatment predictable.
Schilder renamed endodontic radiolucencies (previously called abscess, granuloma, or cyst) lesions of endodontic origin (LEOs) and suggested the biologic job of the endodontic clinician is to prevent or heal LEOs.
Schilder was the first to assign a finishing checklist to radicular shapes. He was the first to be perhaps arrogant enough to suggest three-dimensional obturation was not only possible but predictable. In the 1970s, authors such as Dr. Angelo Sargenti claimed it was impossible to clean the root canal system, and that it was better to “fumigate” the anatomy with formaldehyde in the form of N2 paste. Meanwhile, teachers like Dr. Frank Weine would have legendary debates with Dr. Schilder about whether to be “short” versus “patent” at the POE sites. Clinically, I have never seen a 3D-sealed endodontic failure.3 All endodontic failures to heal were failures to seal.
When I was in dental school at the University of Washington, endodontics originated with Dr. John Ingle who is one of the all-time quintessential teachers, educators, and visionaries of endodontics. He was the first to understand the need fora system-based endodontics. This idea is not new. At that time, it was thought that if the main canal were treated successfully, that a 93 to 95% endodontic success rate could be expected. However, in graduate school at Boston University Henry M. Goldman school of Dental Medicine, Dr. Schilder had a different way of thinking. He said that all root canal system anatomy was potentially significant. Simply treating the “main” canal may simply not be enough. Who was right?
I was about to find out. As an educator, I have always taught that the best education in the world is our own personal education.4-9 So, when I was a 1-year endodontist fresh out of graduate school, a patient named Lucille presented at my office. Her diagnosis and treatment changed my endodontic life forever. Lucille represented a defining moment in my endodontic career. I have never looked back. What did Lucille teach me?
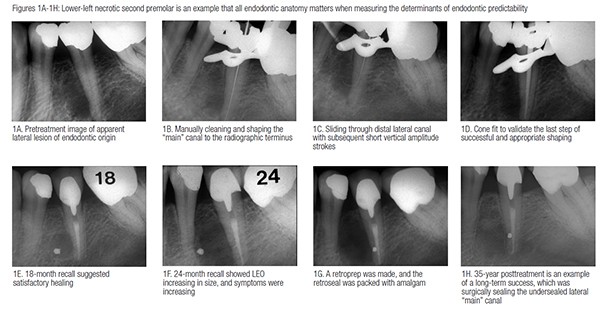
Lucille was referred by her restorative dentist for evaluation of a “lateral radiolucency” distal to her mandibular left second premolar (Figure 1A). The pulp tested nonvital using the electric pulp tester and confirmed using ice test. The pulp did not respond to either test, which suggested a necrotic pulp. The adjacent pulps and contralateral tooth tested vital to the same two tests. The gingival crevice probed within normal limits. In order to confirm necrotic pulp diagnosis, I performed a “test cavity,” which also proved negative. I, therefore, scheduled nonsurgical endodontic treatment. I cleaned and shaped both the “main” root canal and serendipitously slid into a distal midroot lateral canal (Figures 1B and 1C). Endodontic treatment was before the advent of the endodontic microscope and before NiTi rotary shaping. A cone fit was made, and the root canal system was obturated using vertical compaction of warm gutta-percha technique (Figure 1D). The main canal appeared filled, and in addition, a lateral canal was filled at the original lateral LEO site. Lucille was seen for posttreatment 18 months later, and I thought Lucille was healing satisfactorily (Figure 1E). At 24 months posttreatment, however, the LEO was increasing in size, and the tooth was becoming symptomatic (Figure 1F). Since the “main” canal appeared properly sealed, and since the LEO was located exclusively lateral, my treatment plan was to attempt to locate and seal the apparent offending undersealed lateral canal. My thinking was that if the lateral LEO then healed, that for Lucille, at least, her “main” canal would have been a lateral canal. If this were true, then Dr. Schilder was right: all anatomy is potentially significant, and I would have my own clinical example to prove that even a lateral canal could be the “main” or significant canal. I would understand for the first time in my own clinical experience that the location of the POEs could influence predictability regardless of their location along the entire root surface. I surgically discovered Lucille’s lateral canal, made a retropreparation using a straight handpiece and surgical length quarter round bur, and placed a lateral retrograde seal with amalgam, which was the surgical seal of choice at the time (Figure 1G). A subsequent 35-year posttreatment image demonstrated regeneration of the apical and lateral lamina dura and periodontal ligament (Figure 1H). Lucille’s mandibular left second premolar remained asymptomatic throughout all those years.
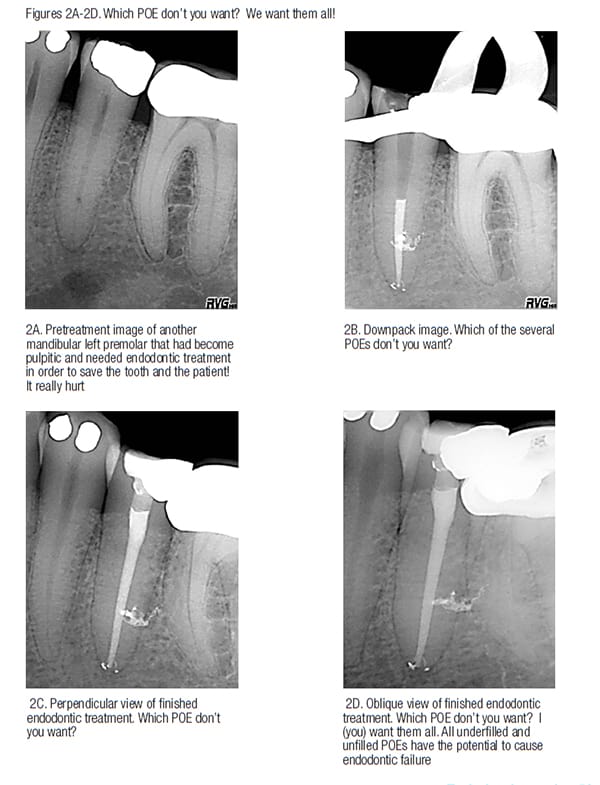
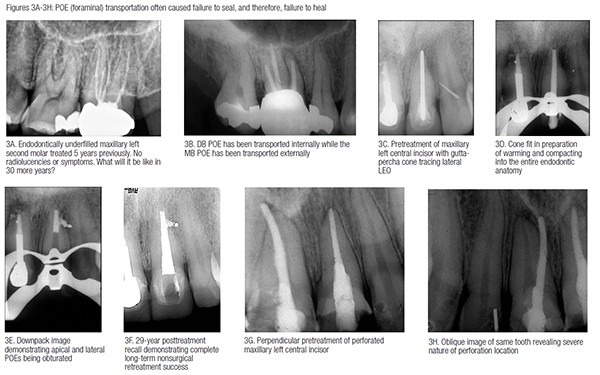
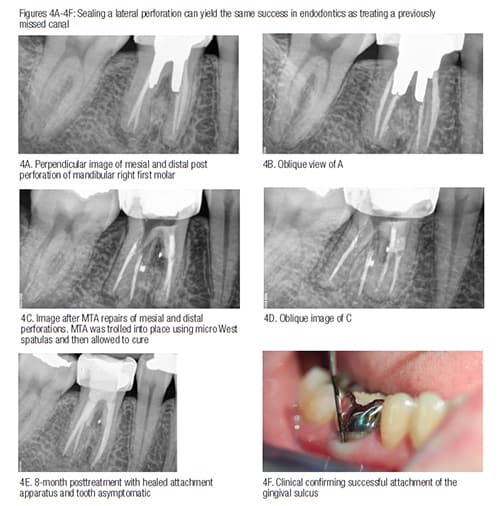
My lesson learned from Lucille was first that there are no POEs that we don’t want (Figures 2A-2D). I also have learned that nature is unpredictable when it comes to underfilled root canal systems that heal or don’t heal (Figures 3A-3H). My final lessonin this issue of Anatomy Matters is that nature heals LEOs in the presence of both mechanical and natural POE perforations (Figures 4A-4F).
So “What’s it all about?” The answer has always been simple: anatomy matters, anatomy matters, and anatomy matters. Measure your successes and failures during your endodontic career by having an intentional long-term treatment recall system. Then look back, see what you have learned, and then become part of the evidence that matters.
 John West, DDS, MSD, the founder and director of the Center for Endodontics, continues to be recognized as one of the premier educators in clinical and interdisciplinary endodontics. Dr. West received his DDS from the University of Washington in 1971 where he is an affiliate associate professor. He then received his MSD in endodontics at Boston University Henry M. Goldman School of Dental Medicine in 1975 where he is a clinical instructor and has been awarded the Distinguished Alumni Award. Dr. West has presented more than 400 days of continuing education in North America, South America, and Europe while maintaining a private practice in Tacoma, Washington. He co-authored “Obturation of the Radicular Space” with Dr. John Ingle in Ingle’s 1994 and 2002 editions of Endodontics and was senior author of “Cleaning and Shaping the Root Canal System” in Cohen and Burns 1994 and 1998 Pathways of the Pulp. He has authored “Endodontic Predictability” in Dr. Michael Cohen’s 2008 Quintessence text Interdisciplinary Treatment Planning: Principles, Design, Implementation, as well as Dr. Michael Cohen’s soon to be published Quintessence text Interdisciplinary Treatment Planning Volume II: Comprehensive Case Studies. Dr. West’s memberships include: 2009 president and fellow of the American Academy of Esthetic Dentistry, and 2010 president of the Academy of Microscope Enhanced Dentistry, the Northwest Network for Dental Excellence, and the International College of Dentists. He is a 2010 consultant for the ADA’s prestigious ADA Board of Trustees where he serves as a consultant to the ADA Council on Dental Practice. Dr. West further serves on the Henry M. Goldman School of Dental Medicine’s Boston University Alumni Board. He is a Thought Leader for Kodak Digital Dental Systems, and serves on the editorial advisory boards for: The Journal of Esthetic and Restorative Dentistry, Practical Procedures and Aesthetic Dentistry, and The Journal of Microscope Enhanced Dentistry. Visit www.centerforendodontics.com, or email: johnwest@centerforendodontics.com, phone 1-800-900-7668 (ROOT), fax 253-473-6328.
John West, DDS, MSD, the founder and director of the Center for Endodontics, continues to be recognized as one of the premier educators in clinical and interdisciplinary endodontics. Dr. West received his DDS from the University of Washington in 1971 where he is an affiliate associate professor. He then received his MSD in endodontics at Boston University Henry M. Goldman School of Dental Medicine in 1975 where he is a clinical instructor and has been awarded the Distinguished Alumni Award. Dr. West has presented more than 400 days of continuing education in North America, South America, and Europe while maintaining a private practice in Tacoma, Washington. He co-authored “Obturation of the Radicular Space” with Dr. John Ingle in Ingle’s 1994 and 2002 editions of Endodontics and was senior author of “Cleaning and Shaping the Root Canal System” in Cohen and Burns 1994 and 1998 Pathways of the Pulp. He has authored “Endodontic Predictability” in Dr. Michael Cohen’s 2008 Quintessence text Interdisciplinary Treatment Planning: Principles, Design, Implementation, as well as Dr. Michael Cohen’s soon to be published Quintessence text Interdisciplinary Treatment Planning Volume II: Comprehensive Case Studies. Dr. West’s memberships include: 2009 president and fellow of the American Academy of Esthetic Dentistry, and 2010 president of the Academy of Microscope Enhanced Dentistry, the Northwest Network for Dental Excellence, and the International College of Dentists. He is a 2010 consultant for the ADA’s prestigious ADA Board of Trustees where he serves as a consultant to the ADA Council on Dental Practice. Dr. West further serves on the Henry M. Goldman School of Dental Medicine’s Boston University Alumni Board. He is a Thought Leader for Kodak Digital Dental Systems, and serves on the editorial advisory boards for: The Journal of Esthetic and Restorative Dentistry, Practical Procedures and Aesthetic Dentistry, and The Journal of Microscope Enhanced Dentistry. Visit www.centerforendodontics.com, or email: johnwest@centerforendodontics.com, phone 1-800-900-7668 (ROOT), fax 253-473-6328.
- Schilder H. Filling root canals in three-dimensions. Dent Clin North Am. 1967;723-44.
- Schilder H. Cleaning and shaping the root canal. Dent Clin North Am. 1974;18(2):269-96.
- West J. The frequency of underfilled root canal systems in endodontic failures. Presented at: Boston University School of Graduate Dentistry; June 1975.
- West J. Anatomy matters. Endodontic Practice US. 2012;5(2):14-16.
- West J. Anatomy matters — part 2. Endodontic Practice US. 2012;5(4):26-27.
- West J. Anatomy matters — part 3. Furcal endodontic seal heals furcal lesion of endodontic origin. Endodontic Practice US. 2012;5(6):22-24.
- West J. Anatomy matters. Long-term case report. Endodontic Practice US. 2013;6(1):50-51.
- West J. Anatomy matters. Root canal system anatomy only matters when it matters. Endodontic Practice US. 2013;6(2):56-58.
- West J. Anatomy matters — part 6. Do lateral canals really matter? Endodontic Practice US. 2013;6(3):52-53.
Stay Relevant With Endodontic Practice US
Join our email list for CE courses and webinars, articles and more..
