CE Expiration Date: September 1, 2025
CEU (Continuing Education Unit):2 Credit(s)
AGD Code: 070
Educational aims and objectives
This self-instructional course for dentists aims to explore a new endodontic file system, the ExactTaperH DC™ file that aims at providing more conservative shaping protocols to practitioners interested in preserving more tooth structure during root canal therapy.
Expected outcomes
Endodontic Practice US subscribers can answer the CE questions by taking the quiz online to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can:
- Realize the importance of being mindful of preserving as much pericervical dentin as possible.
- Recognize the importance of adopting dentin conservation principles with a protocol that creates space for irrigant exchange while also providing resistance form in the apical one-third allowing for obturation control.
- Identify some characteristics of the ExactTaperH DC file that can provide more conservative shaping protocols.
- View two case reports, one instrumented in a conservative manner and one where too much pericervical dentin was removed.
Dr. Mark Anthony Limosani takes a close look at ExactTaperH DC™ endodontic files and their ability to preserve tooth structure during root canal therapy.
Dr. Mark Anthony Limosani discusses a new endodontic file system
Endodontic therapy’s primary purpose is to optimize oral health by preserving the natural dentition by treating an ailing pulp dentin complex. Most practitioners are mindful of the fact that the longevity of their work depends on the patient’s ability to manage oral hostilities such as caries, periodontal disease, and occlusal disharmony, just to name a few. The practitioner’s primary objective in attempting to preserve the natural dentition that has succumbed to pulpal disease is to extirpate inflamed and infected tissue from the root canal system, thus decreasing the biological burden to a level that no longer triggers an immune response. Care must be taken subsequently to restore the damaged dentin-enamel complex to a level where predictable masticatory function can resume without discomfort or clinical manifestations of disease. The main procedural challenge one encounters is striking a balance between achieving all biological goals aforementioned without weakening the tooth from a structural perspective. This article’s purpose is to bring to light a new endodontic file system, the ExactTaperH DC™ file (SS White Dental®, Lakewood, New Jersey) that aims at providing more conservative shaping protocols to practitioners interested in preserving more tooth structure during root canal therapy.
Clark and Khademi outlined the hierarchy of tooth needs emphasizing the importance of being mindful of preserving as much pericervical dentin as possible at the expense of tooth structure that offers less structural support.1 Access design and shaping principles aimed at fulfilling this goal will often leverage carious or previously restored areas of the tooth in order to facilitate instrumentation while also minimizing mechanical compromise. The ExactTaperH DC System allows the practitioner to adopt dentin conservation principles with a protocol that creates space for irrigant exchange while also providing resistance form in the apical one-third allowing for obturation control.
Several elements have been put into practice to allow for the creation of this series of files that allow for the principles of dentin preservation to come to life. First, the heat-treated nature of the nickel-titanium instruments has allowed for a significant increase in flexibility thus providing more resistance to cyclic fatigue. Second, the heat-treated nature of the files has allowed them to maintain shape memory, which allows for them to be precurved prior to their insertion into the canal space. These features have become critical when performing root canal therapy on patients with limited openings where traditional instruments would be a much greater risk of separating during the procedure, creating a whole host of issues for the practitioner.
Another component that plays into the ExactTaperH DC System’s ability to fulfill on its promise of greater dentin conservation resides in the variable taper design combined with a restricted maximum flute diameter. Previous file designs involved a constant taper from D1 to D16, thus removing more tooth structure in the coronal one-third of the canal space. The ExactTaperH DC System allows for the most tapered portion of the instrument to be concentrated in the apical one-third of the file. The taper of the file then diminishes in the midroot and coronal aspect allowing for increased flexibility and preservation of root structure. Such properties decrease the possibility of unintended alteration of the internal anatomy of the tooth, sometimes leading to complications such as apical transportation, ledging, or strip perforation. The maximum flute diameter is defined as the cutting area of the file with the widest width. Traditional file designs presented a MFD of 1.2 mm compared to the ExactTaperH DC’s significantly more conservative 0.8 mm. This decrease in shape becomes all the more crucial when dealing with teeth with longer roots and/or a more delicate slender body.
Case report 1
A 42-year-old female patient presented to the office with a constant throbbing sensation associated with the right aspect of her jaw. She reported having had tooth No. 31 restored with full cuspal coverage slightly over 2 weeks prior due to complaints of biting sensitivity at the time. Tooth No. 31 was diagnosed with symptomatic irreversible pulpitis and normal apical tissues as she presented a lingering response to the cold test. The bitewing radiograph revealed a restoration that appeared to be moderately close to the pulp chamber of tooth No. 31 (Figure 1).
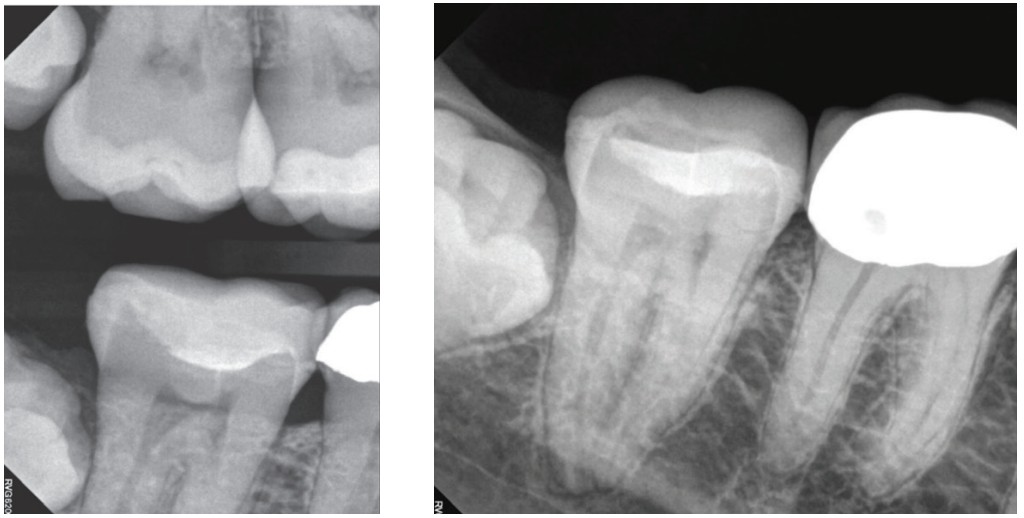
The periapical radiograph of tooth No. 31 revealed roots that appeared to be longer than most as well as proximity of the apices to the M and D roots (Figure 2). Endodontic access was performed through the ceramic restoration using a round SS White Dental® Great White® Gold Bur as well as a coarse grit chamfer diamond to enter the pulp chamber. A hyperemic pulp was noted. Note the conservative nature of the access design aimed at minimizing removal of valuable tooth structure (Figure 3).

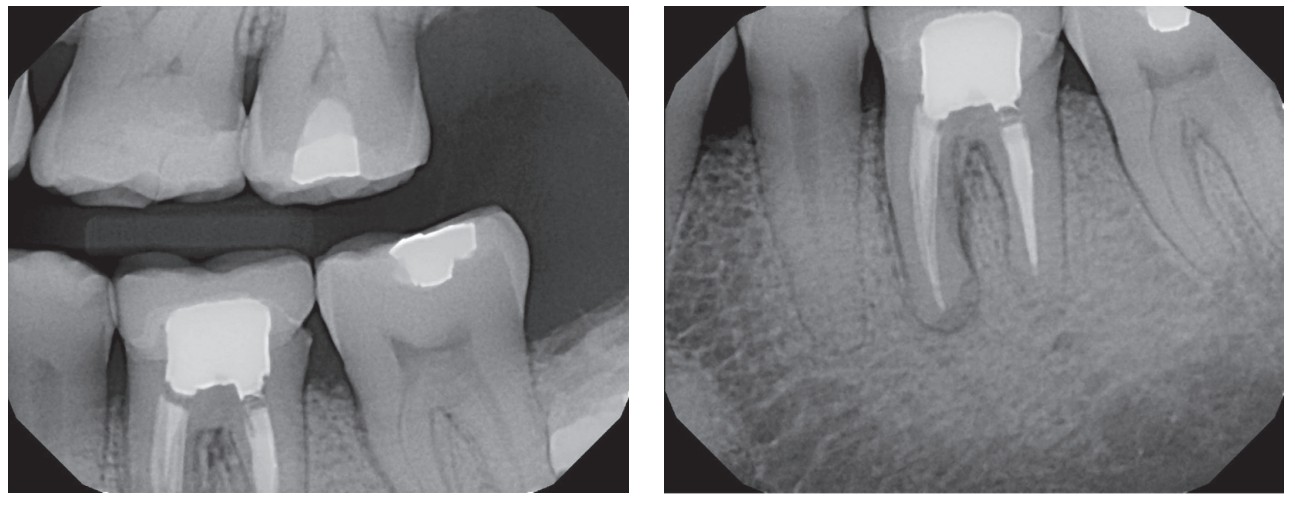
The final radiograph demonstrates the root canal system obturated with Endosequence® BC Sealer™ (Brasseler USA®, Savannah, Georgia) using thermomechanical compaction in the D root along with a single-cone obturation in the M root system. MF cones were used in all canals (Figure 4). The system was disinfected using the GentleWave® system along with the CleanFlow™ handpiece (Sonendo®, Laguna Hills, California). Radiopaque findings consistent with impacted teeth Nos. 1 and 32 were noted. The patient reported that she had been recommended to have these teeth extracted in the past; however, she was recently advised to keep them under observation due to the possible complications related to their proactive removal. The off-angle radiograph reveals two M canals obturated with conservative shapes in a predictable manner (Figure 5). All canals were instrumented using the following sequence with the ExactTaperH DC instruments: 14.03, 17.03, 18.04, and 20.06.

Case report 2
The value of pericervical dentin has been reported.2,3 Pericervical dentin has been defined as root structure residing in proximity to the cervical crest of bone. This zone was often compromised in the past by overflaring the root canal system in an attempt to provide easier access to the midroot and apical one-third of the canal. While shaping the canal system in this manner can facilitate the practitioner’s ability to create a pathway to the apex of the tooth, it often comes at the expense of healthy root structure, thus potentially compromising long-term function.
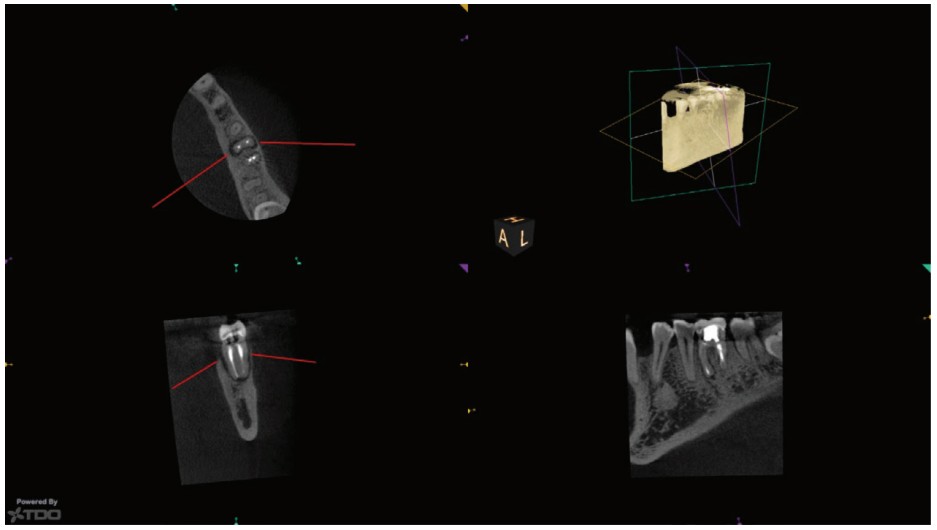
An example of removing too much cervical dentin can be seen in the case of this 51-year-old male who presented with swelling associated with the B aspect of the M root of tooth No. 19. The bitewing radiograph demonstrates findings suggestive of a straight line access design combined with more pronounced coronal shaping (Figure 6). The PA radiograph demonstrated findings suggestive of significant midroot and coronal root shaping during initial treatment (Figure 7). Frontal and axial CBCT slices taken with a CS 8100 3D (Carestream Dental, Atlanta, Georgia) reveal findings highly suggestive of bone loss associated with the M aspect of tooth No. 19 consistent with a fractured root (Figure 8).
Conclusion
As endodontists, we typically have other files that we use in our armamentarium, but I find that this endodontic file provides a balanced combination of optimized metallurgy, conservative maximum flute diameter, and variable taper, allowing for practitioners of all skill levels to embark on a journey of dentin conservation. This system provides dentists and root canal specialists alike with an armamentarium that empowers them to accomplish all their biological endodontic objectives without compromising the structural integrity of their patient’s natural dentition.
Read Dr. Gregori Kurtzman’s article, “Restorative-driven endodontics for more conservative outcomes,” to see a case study of his use of ExactTaperH DC™. https://endopracticeus.com/restorative-driven-endodontics-for-more-conservative-outcomes/
Author Info
 Mark Anthony Limosani, DMD, MS, FRCD(c), received his DMD degree from the University of Montreal in 2007. He attended the specialty program in endodontics at Nova Southeastern University where he also received his master’s degree in dental science. He is a Fellow of the Royal College of Dentists of Canada and a Diplomate of the American Board of Endodontics. He is currently on staff at Miami Children’s Hospital and teaches at the AEGD residency program at Community Smiles. Dr. Limosani has lectured locally and internationally on dental traumatology, restoration of endodontically treated teeth, restoratively minded endodontics, diagnosis and treatment planning, and cone beam computed tomography (CBCT) use in endodontics.
Mark Anthony Limosani, DMD, MS, FRCD(c), received his DMD degree from the University of Montreal in 2007. He attended the specialty program in endodontics at Nova Southeastern University where he also received his master’s degree in dental science. He is a Fellow of the Royal College of Dentists of Canada and a Diplomate of the American Board of Endodontics. He is currently on staff at Miami Children’s Hospital and teaches at the AEGD residency program at Community Smiles. Dr. Limosani has lectured locally and internationally on dental traumatology, restoration of endodontically treated teeth, restoratively minded endodontics, diagnosis and treatment planning, and cone beam computed tomography (CBCT) use in endodontics.
Disclosure: Dr. Limosani has received lecture honorarium from SS White Dental® for courses on endodontics
References
- Clark D, Khademi J. Modern molar endodontic access, and directed dentin conservation. Den Clin North Am. 2010;54(2):249-273.
- Makati D, Shah NC, Brave D, et al. Evaluation of remaining dentin thickness and fracture resistance of conventional and conservative access and biomechanical preparation in molars using cone-beam computed tomography: An in vitro study. J Conserv Dent. 2018;21(3):324-327.
- Haralur SB, Al-Qahtani AS, Al-Qarni MM, Al-Homrany RM, Aboalkhair AE. Influence of remaining dentin wall thickness on the fracture strength of endodontically treated tooth. J Conserv Dent. 2016;19(1):63-67.
Stay Relevant With Endodontic Practice US
Join our email list for CE courses and webinars, articles and more..
