CE Expiration Date:
CEU (Continuing Education Unit): Credit(s)
AGD Code:
Educational aims and objectives
This article aims to present an analysis of fractures of instruments.
Expected outcomes
Endodontic Practice US subscribers can answer the CE questions by taking the quiz to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can:
- Identify successful effective approaches to remove two different instruments from root canals while limiting the loss of tooth structure during removal.
- Recognize several factors can attribute toward instrument failure.
- Realize the benefit of the use of the dental operating microscope in these situations.
- Identify various techniques and equipment for instrument removal from root canal systems.
- Realize the need for careful consideration of the creation of a staging platform when using certain techniques.
Editor’s intro: Drs. Jonker and van der Merwe report on how to effectively remove fractured endodontic instruments.
Drs. Casper H. Jonker and Carel (Boela) van der Merwe report on treatments for this stressful and unpleasant situation for endodontists
Abstract
The separation of an endodontic instrument within the root canal system can be one of the most stressful and unpleasant situations with which the clinician can be confronted. These fractures often occur due to incorrect use of instruments. The clinician is confronted with a few options when considering this situation. These options can include leaving the fragment where the fracture occurred and incorporating the fragment to form part of the final obturation or removal from the root canal. Once the decision is made to remove the fractured instrument, the clinician must realize that the procedure can be one of the most difficult treatments to attempt. According to the literature, there is no standardized method to follow when attempting to remove fractured instruments. The presented cases illustrate effective techniques to remove fractured endodontic instruments from the root canal system. Two cases are discussed where fractured instruments are removed using various manual instruments, ultrasonics, chemicals, and the dental operating microscope (DOM). Satisfactory endodontic outcomes were achieved, and the fractured instruments were successfully removed without causing iatrogenic damage to the remaining tooth structure.
Introduction
Root canal treatments are attempted with the knowledge that certain unforeseen accidents can occur during any part of the treatment. These accidents can include fracture of instruments, perforation of the root on different levels, and the formation of ledges. Once a tooth is exposed to procedural accidents and unforeseen complications, there is an increased risk of failure of the endodontic treatment and reduction of long-term prognosis (Iqbal, 2016; Sjögren, et al., 1990; Siqueira, 2001). The complete treatment can be jeopardized from the cleaning and shaping sequence to the ultimate obturation and 3D sealing of the root canal system (Sjögren, et al., 1990; Siqueira, 2001). The reason why a root canal treatment is performed is to eliminate microorganisms within the root canal system, removal of necrotic or infected pulp tissues, and complete sealing of the root canal spaces (Iqbal, 2016).
The separation of an endodontic instrument within the root canal system can be one of the most stressful and unpleasant situations with which the clinician can be confronted. These fractures often occur due to incorrect use of instruments. Operators can utilize incorrect movements during cleaning and shaping or use deformed instruments, pushing them beyond their ability to absorb the workload (Grossman, 1969; Parashos, et al., 2004). Once an instrument fractures, a detailed approach should be followed to assess the possibility of removal. The clinician should be thoroughly aware of the complicating factors when attempting the removal. These factors may include the following:
- the unique anatomy of the root canal system
- the availability of materials, instruments, and devices to dislodge and remove separated instruments
- the clinician’s experience and ability
- the location, size, position, and diameter of the fractured portion (Parashos, et al., 2004; Suter, et al., 2005)
The treating clinician is confronted with a few options when considering an approach. These options are leaving the fragment where the fracture occurred and incorporating the fragment to form part of the final obturation or attempting removal from the root canal (Saunders, et al., 2004). There is also an alternative technique that can be considered — namely, “bypass” of the separated fragment. Although a tedious exercise, creating space and inserting a small manual file between the fragment and the root canal may lead to full working-length negotiation. Occasionally, the fragment can be loosened and removed during bypassing, but often the fragment remains in situ, ending up forming an integrated part of the final obturation (Saunders, et al., 2004).
Once the decision is made to remove the fractured instrument, the clinician must realize that the procedure can be one of the most difficult treatments to attempt (Saunders, et al., 2004). According to the literature, there is no standardized method to follow when attempting to remove fractured instruments (Frota, et al., 2004). The importance of proper vision, illumination, and magnification cannot be emphasized enough when attempting retrieval (Hülsmann, 1994; Gencoglua and Helvacioglub, 2009). The dental operating microscope (DOM) can create direct visualization of the fractured instrument fragment deep in root canals where normal vision is inadequate (Shiyakov and Vasileva, 2014).
The following case presentations aim to describe an effective approach to remove a fractured instrument using documented techniques and a combination of instruments and equipment, including manual fine ultrasonic tips, small-sized manual files, and the DOM.
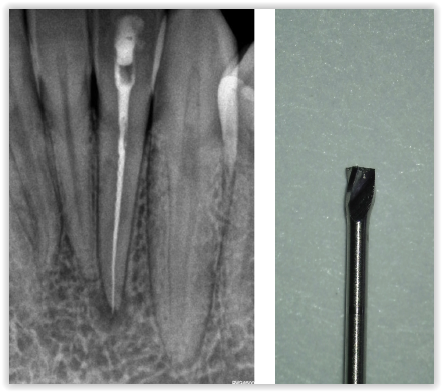
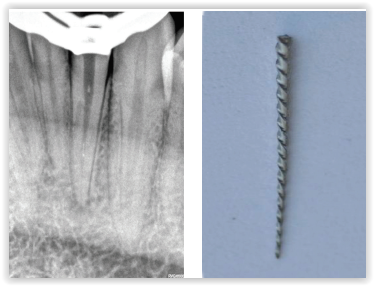
Figures 1 and 2: 1. Preoperative radiograph revealing a large fragment of a fractured instrument in the mandibular second incisor. 2. Magnified image of the modified head of the size 3 Gates Glidden bur used to create the staging platform
Case report 1
A 31-year-old female patient with an uncomplicated medical history reported with a referral letter from a nearby practice requesting removal of a fractured instrument from her mandibular second incisor. The clinician fractured an instrument during cleaning and shaping and incorporated the fragment into the final obturation. The patient developed discomfort after a period of time, and after discussion with the treating clinician, the patient was referred for removal of the fragment. A preoperative radiograph was taken, and it was noted that a large portion of an endodontic instrument fractured inside the root canal with extrusion beyond the apical foramen (Figure 1).
Possible complications were explained before any treatment was carried out. The tooth was anesthetized and the restoration removed to expose the obturation material. Gutta percha was removed to the level of the fractured instrument using a combination of solvents (Chloroform BP, Medicolab, Johannesburg, South Africa) and K-files. The dental operating microscope (DOM) (Carl Zeiss, Oberkochen, Germany) was used to obtain straight line access and visualize the fractured instrument. A staging platform was created by altering a No. 3 Gates Glidden bur (Dentsply Sirona Endodontics, Ballaigues, Switzerland) (Figure 2) to the level of the coronal portion of the fragment.
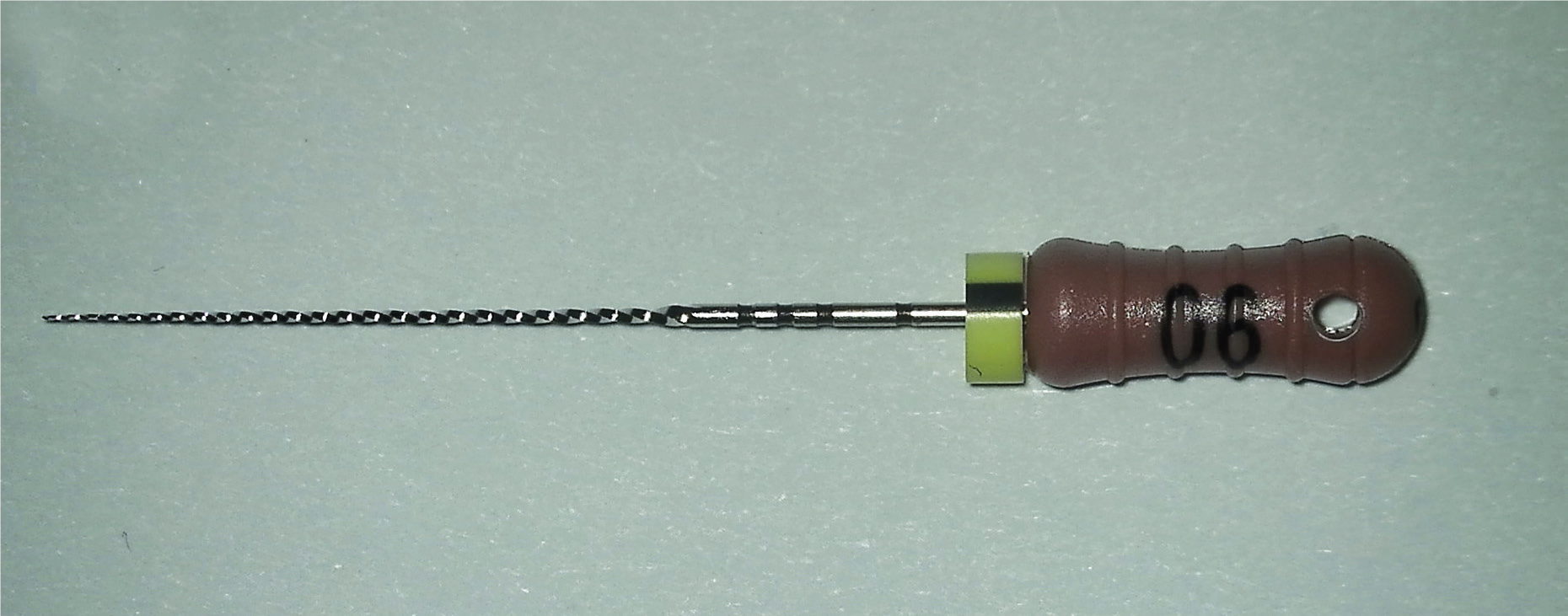
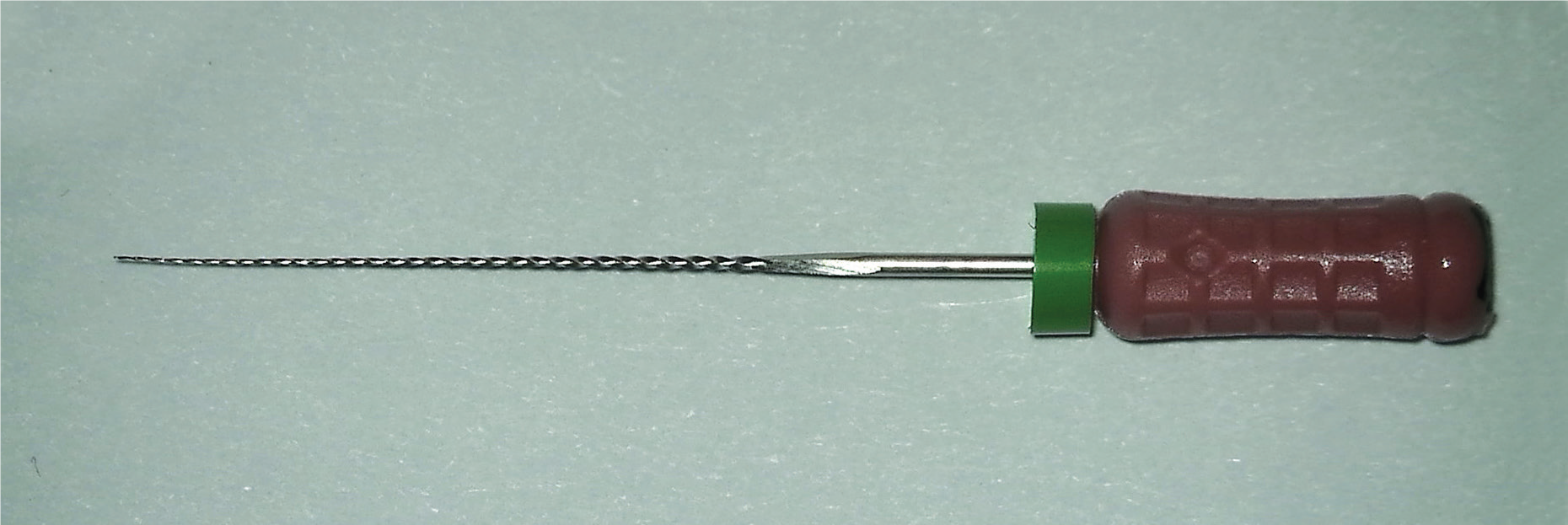
The root canal space was flooded with 17% liquid EDTA (Vista Dental Products, Racine, Wisconsin) and activated using the ultrasonic E7 tip (NSK, Kanuma Tochigi, Japan) in an effort to remove debris and inorganic matter and improve visualization of the fragment. The tip was placed on the coronal part of the fractured instrument and activated on a low setting of 3 on the ultrasonic unit (NSK, Kanuma Tochigi, Japan). This sequence was repeated 4 times to ensure proper removal of debris in the coronal region of the fractured instrument. The canal was dried and a 0.6 C+ file (Dentsply Sirona Endodontics, Ballaigues, Switzerland) (Figure 3A) was introduced in a gentle pecking motion with slight apical pressure, ultrasonic activation, and viscous 15% EDTA paste (Glyde®, Dentsply Sirona Endodontics, Ballaigues, Switzerland) as a lubricating agent. Ultrasonic energy was transferred to the small hand instruments by placing an ultrasonic tip against the shaft of the file. Once slight apical progression was noted, the 0.6 C+ file was removed, and a 0.6 K-file (Dentsply Sirona Endodontics, Ballaigues, Switzerland) (Figures 3B and 3C) was introduced and used in a similar technique to allow apical progression.
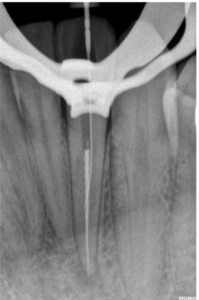

A simultaneous action of gentle pulling, sideways pressure and ultrasonic vibration transferred from the small hand instruments to the fragment was used in an effort to loosen and move the segment in a coronal direction. The preceding sequence was repeated until full working length was reached with the size 0.6 (Figures 4 and 5).
Once movement of the fractured instrument could be observed under magnification, the engaged K-file was tightened by gently rotating the file in a clockwise direction until sufficient resistance was created, and the file was tightly engaged around the segment. A gentle pulling motion with lateral pressure was used in an effort to remove the fractured instrument. The engagement created sufficient resistance to lift the fractured instrument coronally and safely remove from the root canal system (Figures 6 and 7).
Case report 2
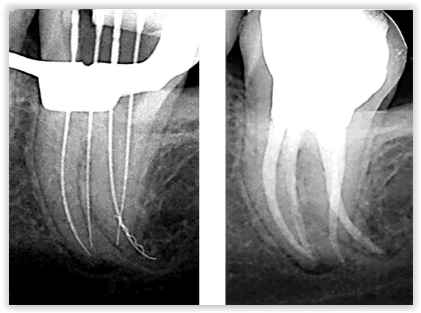
A patient with uncomplicated medical history was referred for the removal of fractured instruments in a mandibular second molar. The preoperative radiograph revealed a fractured instrument in the shape of a Lentulo spiral filler in the disto-buccal canal (joining in the apical third with the disto-lingual canal) as well as a fractured endodontic instrument in the mesio-buccal canal (Figure 8). Periapical radiolucencies were noted on both roots. The tooth was obturated by the referring clinician 4 years ago incorporating the fractured instruments, but the patient developed discomfort over time. After possible complications of the suggested treatment were explained, the tooth was anesthetized, and rubber dam isolation was achieved.
A No. 1 Gates Glidden bur (Dentsply Sirona Endodontics, Ballaigues, Switzerland) with a flooded root canal space with 90% chloroform (Chloroform BP, Medicolab, Johannesburg, South Africa) was used to soften the gutta percha. A No. 0.6 C+ file (Dentsply Sirona Endodontics) was used to create a pathway to the level of the fractured instrument, and softened coronal gutta percha was removed (Figure 9).


A similar technique as described in case report 1 was used to bypass and remove the fragment in the mesio-buccal root. In the disto-buccal root, a similar technique was followed to scout for space around or through the fractured spiral filler and reach full working length. The 0.6 C+ file sequence was followed by a precurved K-file sequence through the fractured fragment until a size 30 K-file (Dentsply Sirona Endodontics, Ballaigues, Switzerland) was reached to full working length. Glyde 15% EDTA paste (Henry Schein®, Melville, New York) was used as lubricating agent, and in between each file sequence, the root canal space was irrigated using 6% sodium hypochlorite (Vista Dental Products, Racine, Wisconsin), patency confirmed with a size 10 K-file (Dentsply Sirona Endodontics, Ballaigues, Switzerland), recapitulation performed, and the root canal re-irrigated to remove debris. A new size 30 Hedstrom file (Dentsply Sirona Endodontics, Ballaigues, Switzerland) (Figure 10) was precurved, and gentle apical pressure was applied in an effort to engage the fragment (Figure 11).
A Steiglitz fractured instrument retrieval forceps (Tinman Dental, Redding, California) was used to lift the fragment coronally using the remaining tooth structure as support. Shaping of all canals was completed using the ProTaper® Universal system (Dentsply Sirona Endodontics, Ballaigues, Switzerland) and all root canals were irrigated in a similar technique as described previously. The canals were dried using large paper points, and a final rinse with 17% liquid EDTA (Vista Dental Products, Racine, Wisconsin) was performed in an effort to remove the smear layer. Obturation was completed using the continuous wave technique with System B™ (Kerr Dental, Orange, California) and Obtura III (Obtura Spartan Endodontics, Algonquin, Illinois) (Figure 12).
Discussion
To encounter instrument fracture in clinical practice is not uncommon. In a survey that was conducted in the United Kingdom where clinicians were ask to report on the incidence of instrument fracture during endodontic treatment, 89% reported that they have experienced the unfortunate event (Madarati, et al., 2008). Several factors can attribute toward instrument failure. These factors can include the creation of inadequate access into the root canal system, anatomical challenges and extreme root curvatures, multiple treatments of the same instrument, and the skill set and experience of the treating clinician (Parashos and Messer, 2006; Nevares, et al., 2012). Varela-Patiño, et al., (2005) also described the importance of glide path preparation to reduce the fracture of endodontic instruments. These authors found that fewer fractures occurred when using rotary instruments when a wide and smooth-walled glide path was created, and the canal was preflared before the introduction of rotary files. In the presented cases, it can be speculated that inadequate access, lack of proper glide path, and increased torsional stress could have attributed to instrument fracture(s), although other factors could also have played a role. Yum, et al., (2011) have concluded that torsional stress and torsional failure are more prevalent in straight canals. Further, the use of spiral fillers must be used with great care in endodontics as they require experience and good tactile sensation to avoid instrument fracture. The instrument possesses a very low fracture resistance to torsional fatigue, and any engagement to the root canal wall can result in instrument separation as observed in case report 2.
The use of the dental operating microscope in endodontics has been advocated by numerous authors in the literature and provided a breakthrough in endodontic treatments. This invaluable piece of equipment has been advocated for the treatment of perforations, removal of fractured instruments, location of orifices, and other applications in endodontics (Castellucci, 2003; Carr and Murgel, 2010; Monea, et al., 2015). Once the decision was made for the removal of a fractured instrument in the presented case, magnification and optimal illumination played a vital role. The creation of the staging platform and use of ultrasonics required proper illumination and magnification and avoid further iatrogenic damage. Further, proper vision under magnification allowed the location of the space between the fractured instrument flutes and created a pathway for small hand instruments (0.6 C+ file and 0.6 K-file).
It can be speculated that without proper vision, the fractured segment could not have been predictably bypassed or removed. One of the treatment options to consider in a case presenting with a fractured instrument is bypassing the segment. Often small manual instruments cannot bypass large fragments, especially when these instruments fractured due to tight contact to the root canal wall. The instrumentation of root canals of smaller diameter generates more torsional stress during the cleaning and shaping procedure than when dealing with root canals of larger diameter (Sattapan, et al., 2000). Attempts to remove these large fragments of fractured instruments with ultrasonics can cause excessive removal of tooth structure and weakening of the root (Nevares, et al., 2012; Madarati, et al., 2010).
In the presented case, a small 0.6 C+ file was used for scouting between the flutes and finding a pathway for small K-files to follow. This instrument was chosen for its unique properties and increased resistance to buckling. Buckling resistance can be defined as elastic lateral deformation when an endodontic instrument is subjected to forces along its axis (Beer and Johnson, 1992). In a study conducted by Lopes, et al., (2012) pathfinding endodontic instruments were compared for buckling resistance. In this particular study, it was found that C+ files showed increased buckling resistance compared to other instruments investigated. In case report 1, the 0.6 C+ instrument managed to bypass the fractured instrument and allowed subsequent instruments for successful removal. It must be emphasized that the C+ file is used for scouting and engagement, but matching size K-files must replace the C+ files once progress is made.
According to the literature, there is no standardized method of instrument removal from root canal systems and often require some initiative from the treating clinician (Hülsmann, 1994; Gencoglua and Helvacioglub, 2009). However, various techniques and equipment have been suggested, including the Masserann kit (Micro-Mega SA, Besancon, France), but even the availability of specialized equipment does not guarantee success. Minimally invasive endodontic access must also be considered when using the Masserann kit. This system must be used with great care in teeth with small diameter roots, curved roots, or where instruments are fractured in the apical region. A great deal of root dentin is removed with increased risk of perforation and root fracture (Pai, et al., 2006). The creation of a staging platform (Ruddle, 1997) with an altered Gates Glidden bur size 3 should be considered as a maximum diameter for the platform. This technique should only be considered in cases where the fractured instrument can be visualized.
Removal of fractured instruments beyond curvatures where no direct vision is possible can be very challenging. There is a high risk of procedural errors and complications, and the creation of a staging platform should be carefully considered. In the present case, an effective approach was followed for removal. It must be emphasized that successful removal of fractured instruments requires an adequate skill set, experience, and thorough understanding of the use of specialized equipment.
Conclusion
The case reports illustrate successful effective approaches to remove two different instruments from root canals while limiting the loss of tooth structure during removal.
This paper is reprinted from International Dentistry – African Edition. 2018;8(5):8-12
Removing fractured endodontic instruments can be stressful for endodontists. Read more about how canal anatomy can play a vital role in instrument fatigue and failure in “Negotiation of an S-shaped canal with an EDM-machined CM instrument: a case report.” https://endopracticeus.com/ce-articles/negotiation-of-an-s-shaped-canal-with-an-edm-machined-cm-instrument-a-case-report/. Subscribers can take the quiz and receive two CE credits!
References
- Beer FP, Johnston. Mechanics of Materials. 3rd ed. New York NY: McGraw-Hill; 1992.
- Carr GB, Murgel, CAF. The use of the operating microscope in endodontics. Dent Clin North Am. 2010;54(2):191-214.
- Castellucci A. Magnification in endodontics: the use of the operating microscope. Pract Proced Aesthet Dent. 2003;15(5):377-384.
- Frota LMA, Aguiar BA, Aragão MGB, de Vasconcelos BC. Removal of Separated Endodontic K-File with the Aid of Hypodermic Needle and Cyanoacrylate. Case Rep Dent. 2016;2016:1-5.
- Gencoglua N, Helvacioglu D. Comparison of the different techniques to remove fractured endodontic instruments from root canal systems. Eur J Dent. 2009;3(2):90-95.
- Grossman LI. Guidelines for the prevention of fracture of root canal instruments. Oral Surg Oral Med Oral Pathol. 1969;28(5):746-752.
- Hülsmann M. Removal of fractured instruments using a combined automated/ultrasonic technique. J Endod. 1994;20(3):144-146.
- Iqbal A. The factors responsible for endodontic treatment failure in the permanent dentitions of the patients reported to the College of Dentistry, the University of Aljouf, Kingdom of Saudi Arabia. J Clin Diagn Res. 2016;10(5):146-148.
- Lopes HP, Elias CN, Mangelli M, et al. Buckling resistance of pathfinding endodontic instruments. J Endod. 2012;38(3):402-404.
- Madarati AA, Watts DC, Qualtrough AJ. Opinions and attitudes of endodontists and general dental practitioners in the UK towards the intracanal fracture of endodontic instruments. Part 1. Int Endod J. 2008;41(8):693-701.
- Madarati AA, Qualtrough AJ, Watts DC. Vertical fracture resistance of roots after ultrasonic removal of fractured instruments. Int Endod J. 2010;43(5):424-429.
- Monea M, Hantoiu T, Stoica A, Sita D, Sitaru A. The impact of operating microscope on the outcome of endodontic treatment performed by postgraduate students. Eur Sci J. 2015;11(27):305-311.
- Nevares G, Cunha RS, Zuolo ML, Bueno CE. Success rates for removing or bypassing fractured instruments: a prospective clinical study. J Endod. 2012;38(4):442-444.
- Pai AR, Kamath MP, Basnet P. Retrieval of a separated file using Masserann technique: a case report. Kathmandu Univ Med J. 2006;4(2):238-242.
- Parashos P, Gordon I, Messer HH. Factors influencing defects of rotary nickel-titanium endodontic instruments after clinical use. J Endod. 2004;30(10):722-725.
- Parashos P, Messer HH. Rotary NiTi instrument fracture and its consequences. J Endod. 2006;32(11):1031-1043.
- Ruddle CJ. Micro-endodontic nonsurgical retreatment. Dent Clin North Am. 1997;41(3):429-454.
- Sattapan B, Palamara JEA, Messer HH. Torque during canal instrumentation using rotary nickel-titanium files. J Endod. 2000;26(3):156-160.
- Saunders JL, Eleazer PD, Zhang P, Michalek S. Effect of a separated instrument on bacterial penetration of obturated root canals. J Endod. 2004;30(3):177-179.
- Shiyakov KK, Vasileva RI. Success for removing or bypassing instruments fractured beyond the root canal curve – 45 clinical cases. J of IMAB. 2014;20(3):567-571.
- Siqueira JF Jr. Aetiology of root canal treatment failure: why well-treated teeth can fail. Int Endod J. 2001;34(1):1-10.
- Sjögren U, Hägglund B, Sundqvist G, Wing K. Factors affecting the long-term results of endodontic treatment. J Endod. 1990;16(10):498-504.
- Suter B, Lussi A, Sequeira P. Probability of removing fractured instruments from root canals. Int Endod J. 2005;38(2):112-123.
- Patiño PV, Biedma BM, Liébana CR, Cantatore G, Bahillo JG. The influence of a manual glide path on the separation rate of Ni-Ti rotary instruments. J Endod. 2005;31(2):114-116.
- Yum J, Cheung GS, Park JK, Hur B, Kim H. Torsional strength and toughness of nickel-titanium rotary files. J Endod. 2011;37(3):382-386.
