CE Expiration Date:
CEU (Continuing Education Unit): Credit(s)
AGD Code:
Educational aims and objectives
This article aims to illustrate how to treat a first molar showing the presence of four canals in the mesial and two canals in the distal root.
Expected outcomes
Endodontic Practice US subscribers can answer the CE questions by taking this quiz to earn 2 hours of CE from reading this article.
Correctly answering the questions will demonstrate the reader can:
- Identify some hints and tips to successfully treatment teeth with multiple roots.
- Identify some statistics on mandibular first molars.
- Realize the unusual nature of a mandibular first molar with four canals in the mesial root.
- Realize the importance of having a good understanding of the canal anatomic complexities to achieve effective disinfection of the root canal system.
- Recognize some imaging technologies that can be used, when appropriate, as an adjunctive tool for detection and management of variable root canal morphology.
This case report, regarding a mandibular first molar with four canals in the mesial root and two canals in the distal root, shows that clinicians need to be aware of the variable morphology of root canals in this tooth.
Drs. Hamed Karkehabadi, Ricardo Machado, and Lucas da Fonseca Roberti Garcia describe a case report of a mandibular first molar showing the presence of four canals in the mesial and two canals in the distal root
Abstract
A 35-year-old female patient with intermittent pain in the lower right jaw was referred to the dental practice. The right mandibular first molar did not respond to thermal testing, and the patient reported moderate pain to percussion and palpation in the region of this tooth. Radiographic findings confirmed the presence of periradicular disease and previous root canal treatment. Initially, only four treated canals were found (two mesial and two distal). Two extra canals were found in the mesial root. The treatment was performed and the success confirmed after 12 months. This case report reiterates the complexity of mandibular first molar variation and is intended to reinforce the clinicians’ need to be aware of the variable morphology of root canals in this tooth.
Introduction
The goal of endodontic treatment is to clean and shape the root canal system and obturate it in all its dimensions (Almeida, et al., 2015). Before starting treatment, aberrant root or root canal morphology should be investigated, detected, and adequately treated (Lea, et al., 2014). Failure to recognize any unusual canal configuration could eventually lead to an unsuccessful treatment outcome (Almeida, et al., 2015; Lea, et al., 2014; Ghoddusi, et al., 2007). Thus, the proper knowledge of the root and root canal morphology, along with any related anatomical variations, is essential to achieve a successful treatment (Almeida, et al., 2015; Lea, et al., 2014; Ghoddusi, et al., 2007).
Mandibular first molars are the teeth that most require endodontic treatment, as they are the first posterior teeth to erupt in permanent dentition (Ghoddusi, et al., 2007). Although mandibular first molars usually have two canals in the mesial root, named as mesiobuccal and mesiolingual canals, the presence of a middle mesial canal in the developmental groove has been widely reported in 1% (Vertucci, 1964), 1.5% (Martinez-Berna and Badanelli, 1983), 2.1% (Fabra-Campos, 1985), 2.6% (Fabra-Campos, 1989), 12% (Pomeranz, et al., 1981), 14.7% (Akbarzadeh, et al., 2017), 15% (Goel, et al., 1991), and 18.6% (Versiani, et al., 2016) of the cases. In addition, mandibular first molars may have one or two canals in the distal root (Ghoddusi, et al., 2007).
As reported in several studies, the prevalence of a middle mesial canal in mandibular first molars may significantly range among researchers. Clinical studies and case reports that demonstrated the presence of negotiable middle mesial canals present different data from studies which used extracted teeth model (Vertucci, 1984; Martinez-Berna and Badanelli, 1983; Fabra-Campos, 1985; Fabra-Campos, 1989; Pomeranz, et al., 1981; Akbarzadeh, et al., 2017; Goel, et al., 1991; Versiani, et al., 2016).
To the best of the authors’ knowledge, just one case has ever been reported in the scientific literature of a mandibular first molar with four canals in the mesial root (Reeh, 1998). In this particular case, the author reported a successful endodontic retreatment of a mandibular first molar with seven canals, where the other three canals were located in the distal root. Initially, the clinician failed in detect the complexity of the root canal system of this tooth, and only three canals were submitted to endodontic treatment. Such factor demonstrates the importance of knowing the root canal system morphology and its anatomical variations (Reeh, 1998). Furthermore, according to the author of the case report, looking for additional canals was crucial for a successful outcome (Reeh, 1998).
Therefore, the aim of this article is to report a clinical case of a mandibular first molar with four canals in the mesial root and two canals in the distal root. All canals were properly prepared and filled, and the success of the treatment was confirmed after 12 months by clinical and radiographic findings.
Case report
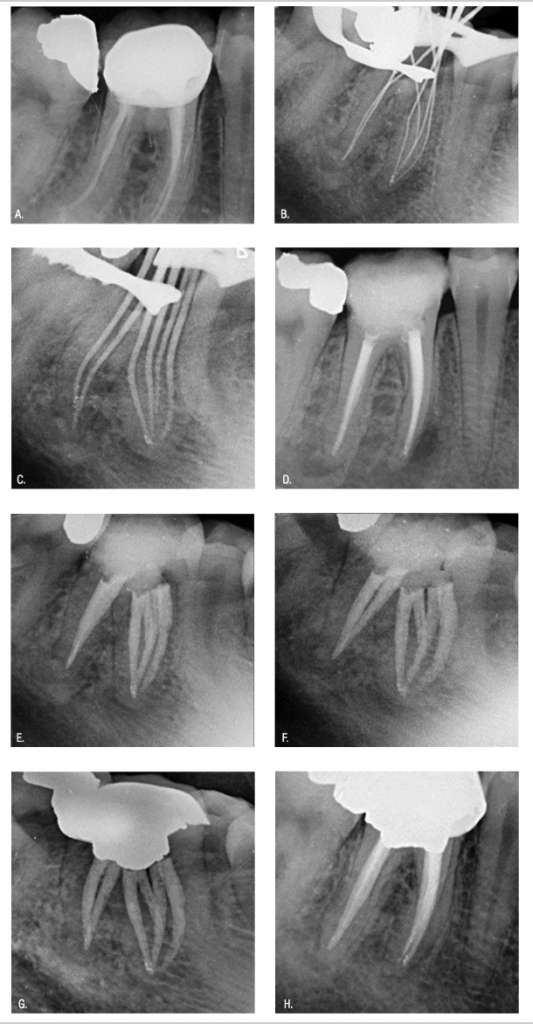
A 35-year-old female patient, with a history of intermittent pain in the lower right jaw 3 weeks previous to being seen, was referred to the dental practice. Medical history was non-contributory. The right mandibular first molar did not respond to thermal testing (heated gutta percha and dry ice), and the patient reported moderate pain to percussion and palpation in the region of this tooth. Furthermore, the tooth had a total crown, and there was no significant probing depth. Radiographic findings confirmed the presence of periradicular disease and previous root canal treatment (Figure 1A). Correlation of clinical and radiographic findings led to a diagnosis of a chronic periradicular abscess due to previous unsuccessful endodontic treatment. Therefore, a nonsurgical root canal retreatment was recommended.
After administrating infiltration anesthesia (Lidocaine 2% 1:80.000 epinephrine), the crown was removed, and rubber dam isolation of the operative area was performed. An endodontic access cavity was prepared by using 1016HL and Endo Z burs (Dentsply Sirona Maillefer), and four previously treated root canals were found. Removal of root canal filling was performed by using a Neoniti A1 size 20 file (Neolix, Châtres-la-Forêt, France). After a careful analysis of the floor of the pulp chamber, two additional root canals were found in the mesial root, totaling four canals in this root. Initially, extra canals were explored with a size 10 K-File (Mani, Inc; Tochigi, Japan) under copious irrigation with 5.25% sodium hypochlorite solution (Chloraxid, Cerkamed, Poland). Next, the working length of each root canal was established 1 mm up to the apical foramen, by using an electronic apex locator (Root ZX, Morita, Tokyo, Japan). Then a radiograph was taken to confirm the measurements (Figure 1B). The chemo-mechanical preparation was performed by the crown-down technique, with the Neoniti system (Neolix). The first four root canals found (MB1, ML1, DB, and DL) were prepared up to a Neoniti A1 size 25 file (Neolix). The two additional root canals found in the mesial root (MB2 and ML2) were prepared up to a Neoniti A1 size 20 file. Irrigation was performed with 2.5 ml of 5.25% sodium hypochlorite solution (Chloraxid) at each change of file, by using a 30-gauge, open-ended needle (Navitip®; Ultradent®, South Jordan, Utah) placed slightly short of the binding point. After a final rinse with MTAD (Dentsply Tulsa), the root canals were dried with sterile absorbent paper points (Dentsply Maillefer, Ballaigues, Switzerland), and a radiograph was taken of the main cones to confirm if they reached the working length (Figure 1C). Afterwards, the canals were filled with gutta percha (Dentsply Maillefer, Ballaigues, Switzerland) and AH Plus® sealer (Dentsply DeTrey, Ballaigues, Switzerland), using the lateral condensation technique. The pulp chamber was properly cleaned to remove the excess of gutta percha and sealer, and it was temporarily restored with a provisional material (Figures 1D-1F).
Clinical and radiographic findings, as there was no painful symptomatology and regression of the periapical lesion, confirmed the success of the proposed therapy. Continued follow-up over 12 months has shown a positive outcome from an endo-dontic perspective (Figures 1G and 1H).
Discussion
The prevention and treatment of apical periodontitis are the main objectives of endodontic therapy (Siqueira and Rôças, 2008). An adequate biomechanical preparation and filling of the root canal system, associated with the placement of a proper coronal sealing, are crucial and should be taken to achieve this goal (Gillen, et al., 2011). Furthermore, all these steps performed during the treatment require a good understanding of the root canal anatomy to attain a successful outcome (Reeh, 1998).
The purpose of this article was to present the case report of a mandibular first molar clearly showing the presence of four canals in the mesial root and two canals in the distal root. The patient was referred to the dental practice because of the persistent symptoms after the first endodontic treatment, at which time, only four root canals were located and treated (two in the mesial root and two in the distal root).
The clinician should keep in mind that the internal morphology of the teeth does not always follow the known standards (Almeida, et al., 2015; Lea, et al., 2014). In this clinical case, the incomplete debridement of the six root canals probably was the cause for the occurrence and perpetuation of the peri-radicular disease (Reeh, 1998). Once all the root canals were located and could be properly negotiated, shaped, and cleaned, the symptoms disappeared, and a 12-month follow-up X-ray showed the consistent healing of the periapical alveolar bone. To locate additional root canals can be a challenging procedure for professionals; for this reason, the findings reported in this clinical case highlight how important it is to have a good understanding of the canal anatomic complexities to achieve effective disinfection of the root canal system (Siqueira and Rôças, 2008).
The clinician should always suspect the presence of additional root canals and investigate further when examining radiographs and/or locating and exploring the canals (Johal, 2001). Although there are inherent limitations, radiographic examination provides a clue to the type of canal configuration present (Hildebolt, et al., 1990).
Previous reports have continuously used imaging technologies, such as spiral computed tomography (SCT) (Gopikrishna, et al., 2006; Aggarwal, et al., 2009) and cone-beam computed tomography (CBCT) (Almeida, et al., 2015; Lea, et al., 2014), as an adjunctive tool for detection and management of variable root canal morphology. These imaging technologies may be helpful in detecting variations of root canals in doubtful circumstances related to unusual root canal anatomy (Gopikrishna, et al., 2006; Aggarwal, et al., 2009; Almeida, et al., 2015; Lea, et al., 2014). Although these imaging modalities offer an insight into the anatomical variations of the root or root canal configuration, they also potentially increase the effective dose of radiation exposure for the patient, often limiting their use (Patel, et al., 2009).
The ALARA (as low as reasonably achievable) principle states that every effort should be made by professionals to keep the patient’s exposure to ionizing radiation as low as practically possible (Farman, 2005). As reported in the present clinical case, the use of radiographic examination associated to an adequate clinical inspection of the floor of the pulp chamber was enough to depict the variable anatomy clearly. For this reason, advanced imaging techniques (SCT and CBCT) did not have to be used to solve this clinical case.
It is also valid to emphasize that other equipment, such as operative microscopes, may be used to facilitate the location and negotiation of additional root canals, improving significantly the quality of the endodontic therapy. Relvas, et al. (2013), have reported a successful endodontic treatment of a maxillary first premolar with three root canals, with the aid of an optical microscope. The authors stated that the use of such technology was fundamental to allow the location of the third root canal, due to the complex internal anatomy of the tooth (Relvas, et al., 2013).
This article provides useful clinical information for performing endodontic therapy in a very complex case, thus contributing to the awareness of another anatomic variant of mandibular molars.
Conclusions
Reports of cases with unusual morphology have an important didactic value. Their documentation may facilitate the recognition and successful management of similar cases, which may require endodontic therapy. This case report reiterates the complexity of mandibular first molar variation and is intended to reinforce the clinicians’ need to be aware of the variable morphology of root canals in this tooth.
The mandibular first molar is also the subject of Dr. Baker’s article, “Endodontic retreatment of a lower right first molar with WaveOne®.” Read all about it here.
References
- Aggarwal VL, Singla M, Logani A, Shah N. Endodontic management of a maxillary first molar with two palatal canals with the aid of spiral computed tomography: a case report. J Endod. 2009;35(1):137-139.
- Akbarzadeh N, Aminoshariae A, Khalighinejad N, et al. The Association between the Anatomic Landmarks of the Pulp Chamber Floor and the Prevalence of Middle Mesial Canals in Mandibular First Molars: An In Vivo Analysis. J Endod. 2017;43(11):1797-1801.
- Almeida G, Machado R, Sanches Cunha R, Vansan LP, Neelakantan P. Maxillary first molar with 8 root canals detected by CBCT scanning: a case report. Gen Dent. 2015;63(2):68-70.
- Fabra-Campos H. Unusual root anatomy of mandibular first molars. J Endod. 1985;11(12):568-572.
- Fabra-Campos H. Three canals in the mesial root of mandibular first permanent molars: a clinical study. Int Endod J. 1989;22(1):39-43.
- Ghoddusi J, Naghavi N, Zarei M, Rohani E. Mandibular first molar with four distal canals. J Endod. 2007;33(12):1481-1483.
- Goel NK, Gill KS, Taneja JR. Study of root canals configuration in mandibular first permanent molar. J Indian Soc Pedod Prev Dent. 1991;8(1):12-14.
- Lea C, Deblinger J, Machado R, Nogueira Leal Silva EJ, Vansan LP. Maxillary premolar with 4 separate canals. J Endod. 2014;40(4):591-593.
- Martinez-Berna A, Badanelli P. Investigacion clinica de molars inferiors con cinco conductos. Boletin de Informacion Dental. 1983;43:27-31
- Pomeranz HH, Eidelman DL, Goldberg MG. Treatment considerations of the middle mesial canal of mandibular first and second molars. J Endod. 1981;7(12):565-568.
- Reeh ES. Seven canals in a lower first molar. J Endod. 1998;24(7):497-499.
- Siqueira JF Jr, Rôças IN. Clinical implications and microbiology of bacterial persistence after treatment procedures. J Endod. 2008;34(1):1291-1301.
- Gillen BM, Looney SW, Gu LS, et al. Impact of the quality of coronal restoration versus the quality of root canal fillings on success of root canal treatment: a systematic review and meta-analysis. J Endod. 2011;37(7):895-902.
- Gopikrishna VL, Bhargavi N, Kandaswamy D. Endodontic management of a maxillary first molar with a single root and a single canal diagnosed with the aid of spiral CT: a case report. J Endod. 2006;32(7):687-691.
- Hildebolt CF, Vannier MW, Pilgram TK, Shrout MK. Quantitative evaluation of digital dental radiograph imaging systems. Oral Surg Oral Med Oral Pathol. 1990;70(5):661-668.
- Johal S. Unusual maxillary first molar with 2 palatal canals within a single root: a case report. J Can Dent Assoc. 2001;67(4):211-214.
- Patel S, Dawood A, Whaites E, Pitt Ford T. New dimensions in endodontic imaging: part 1. Conventional and alternative radiographic systems. Int Endod J. 2009;42(6):447-462.
- Farman AG. ALARA still applies. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005;100(4):395-397.
- Relvas JB, de Carvalho FM, Marques AA, Sponchiado EC Jr, Garcia Lda F. Endodontic treatment of maxillary premolar with three root canals using optical microscope and NiTi rotatory files system. Case Rep Dent. 2013;710408.
- Versiani MA, Ordinola-Zapata R, Keleş A, et al. Middle mesial canals in mandibular first molars: A micro-CT study in different populations. Arch Oral Biol. 2016;61:130-137.
- Vertucci FJ. Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol. 1984;58(5):589-599.
