CE Expiration Date: June 10, 2024
CEU (Continuing Education Unit):2 Credit(s)
AGD Code: 070
Educational aims and objectives
This self-instructional course for dentists aims to show information regarding endodontic irrigation as well as details regarding a new technique.
Expected outcomes
Endodontic Practice US subscribers can answer the CE questions by taking the quiz to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can:
- Realize the factors that can cause irrigation failures during RCT.
- Recognize some of the more recent systems in the marketplace for endodontic irrigation.
- Realize some ramifications of inflamed pulp remnants.
- Observe a novel in vitro irrigation model.
- Realize the effect of different variables like concentration, temperature, and aeration on the dissolution efficacy of sodium hypochlorite.
Dr. L. Stephen Buchanan introduces a new concept in endodontic irrigation. Read all about it, and then take the quiz to receive 2 CE credits!
Dr. L. Stephen Buchanan discusses a new concept in endodontic irrigation
Endodontic irrigation is the most important part of root canal therapy (RCT), but I confess it has never been the most interesting part of the process for me because there is so little to see going on during irrigation.
All the other aspects of RCT have an easily visualized representation of procedural events — whether that is by direct magnified sight or indirectly, by mental visualization. When I am cutting tooth structure with a diamond bur spun at 200,000 RPM, I see most everything happening at the bur/tooth interface. When I’m directing a rotary file to cut through a canal, even when the file is mostly buried in the root, mentally visualizing the hidden part of the file is very straightforward as I know the file’s geometry, and I know the depth in the canal to which that file’s geometry has progressed. Having cut a 30/.06 rotary file within a millimeter of the canal terminus, I only need to view the instrument’s flute spaces to see where the file cut dentin in the canal, and I can clearly see the hidden surfaces of the just-shaped canal in my mind. Irrigation not so much.
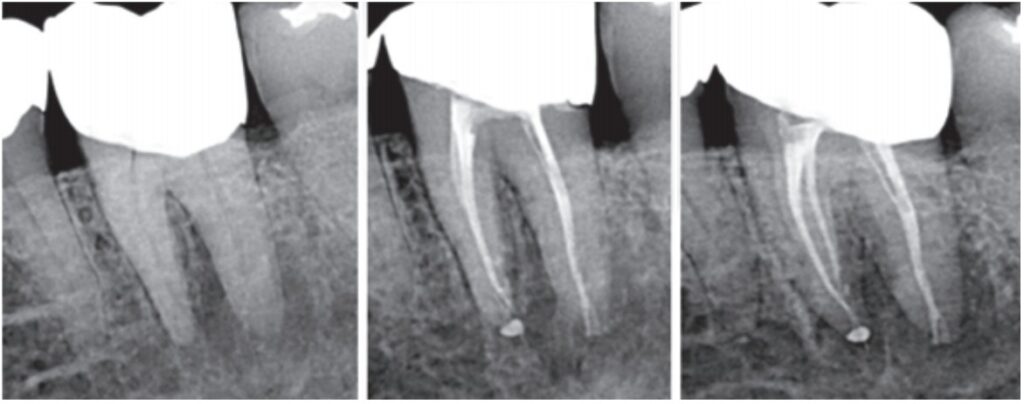
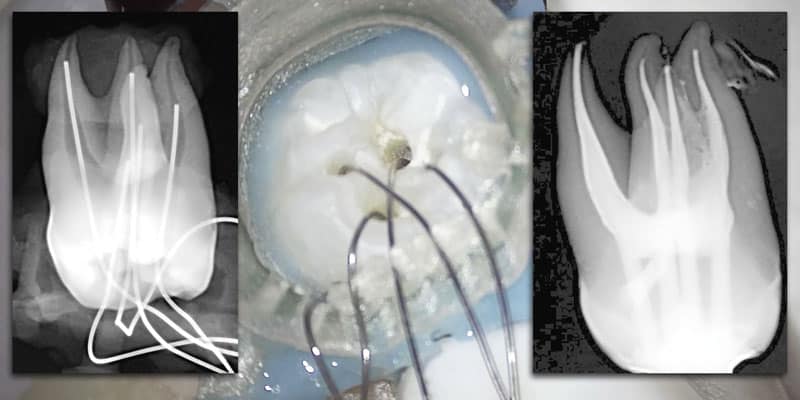
Endodontic irrigation is now the most interesting procedural topic in the field, primarily because of two of the most recent entries into the market — GentleWave® (Sonendo) and BioLase irrigation activation procedures. GentleWave irrigation system forged new ground in endodontics, and both these are able to result in radically smaller instrumentation procedures. We are now seeing a remarkable number of lateral canal irregularities in vital cases — cleaned and filled through preparations as small as 13-.03. More often than not these treatment results look more like one of Walter Hess’ anatomic castings1 than the overcut RCT results we used to associate with excellence in endodontics (Figure 1).
Fear inflamed pulp remnants
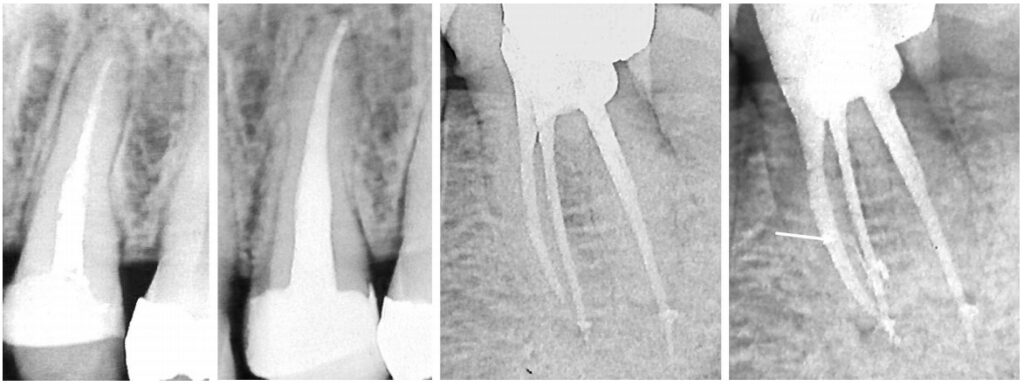
Irrigating canals aside, diagnosing irrigation failures can be very mysterious, and patients unlucky enough to have an incompletely treated tooth containing inflamed pulp remnants are also at great risk of receiving unnecessary RCT and extractions if a diagnostic failure follows. A well-done study2 showed 11% of patients in pain who saw an endodontist were not relieved of their pain within 6 months. Half of these didn’t need an RCT — they had myofascial pain; the other half needed a root canal (better); but half of these had RCT done on the wrong tooth, leaving the last quarter of these pain management failures to irrigation failures such as the cases in Figure 2.
Several factors obfuscate diagnoses of irrigation failures. Start with the fact that pain referred from inflamed pupal remnants may refer to any teeth on the same side of the patient’s face, while percussing the offending tooth may elicit a different awareness at most. The first big tip-off — if you did thorough thermal pulp testing before entry — is the knowledge that treating the tooth alleviated the patient’s thermally induced pain, leaving the patient with spontaneous pain that can be severe. The surprising aspect is how long pulp remnants can stay alive, a function of their close proximity to the rich periradicular blood supply. There will seldom be PR lucencies visible in CBCT volumes, and they won’t get even slightly better on the most effective antibiotics like Augmentin or clindamycin. The diagnosis is made by reviewing the patient’s history and finding notation of severe pulpitis before the emergency access. Give the patient 400 mg of naproxen (Aleve®), wait 40 minutes, and if the pain has been relieved, schedule the patient for the retreat. And do a better job of irrigating the second time.
Deliquesce the pulp
How long does it take to deliquesce (dissolve) an inflamed pulp out of a complex root canal system? Researchers have done many in vitro and ex vivo studies of canalar biofilms3, and while some understand the mission better than others, they have a pretty good idea of what it takes and how long it takes to kill most or all the bugs in a root canal. Regarding pulp tissue in lateral recesses, however, it is generally agreed that it is more difficult and takes longer to digest pulp in lateral recesses than it does to kill biofilm in a pool of slime.
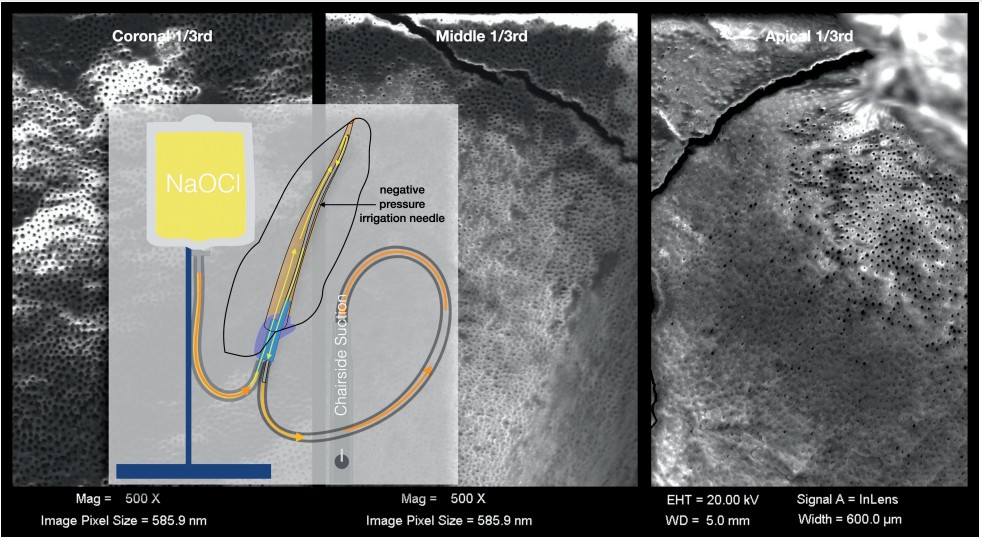
The best pulpal irrigation studies have been done in teeth slated for extraction, splitting their roots open after delivery and using a SEM to view the exposed surfaces (Figure 3) or embedding, slicing, and viewing sections through a light microscope to view the canalar contents. I was inspired to design a novel in vitro irrigation model (Figure 4) by a surprising irrigation failure I had using the multisonic ultracleaning technology5 in a lower C-shaped molar. The most likely etiology I could figure for the tooth to remain sensitive after completion was inflamed pulp fragments remaining in the broad buccal isthmus between the MB and D canals. The first time an isthmus dissolution study was done in this new model that, theory was confirmed (Figure 5); at the end of the 5-minute NaOCl cycle, pulp analog remained.
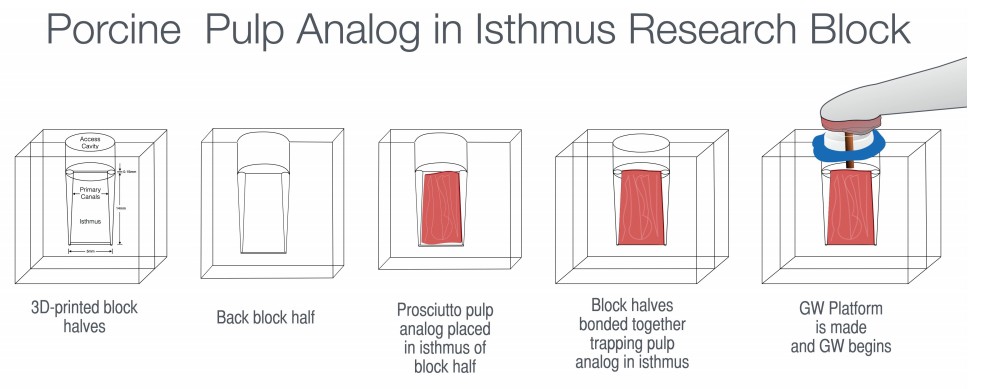
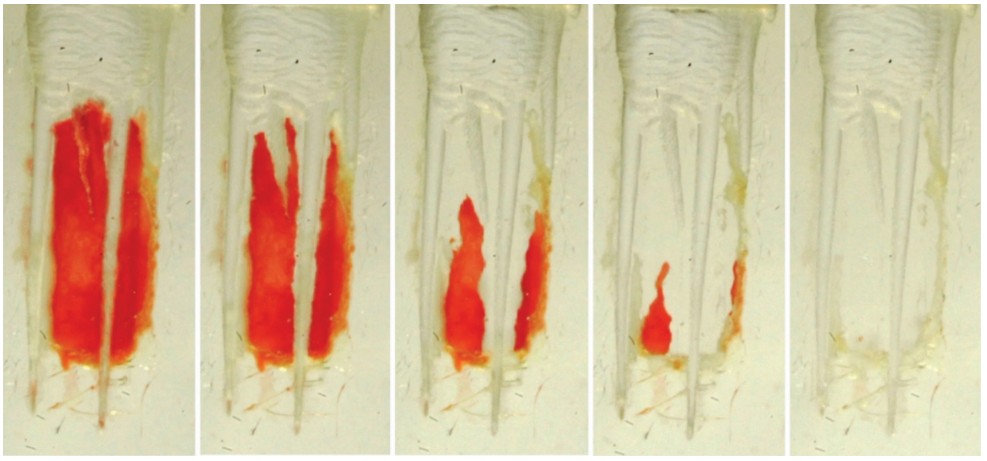
Watching playbacks of the video recording through the clear isthmus block, as the prosciutto captured between the block halves was irrigated and digested by NaOCl, fascinated me, especially when I realized I could watch how different variables like concentration, temperature, and the surprise variable aeration effected the dissolution efficacy of sodium hypochlorite (Figures 5-7).
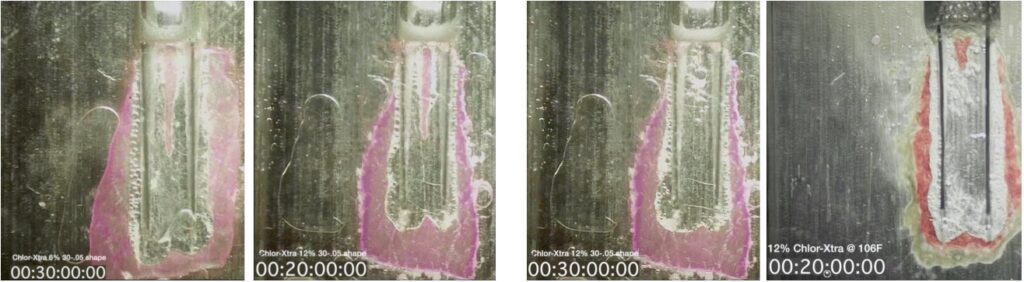
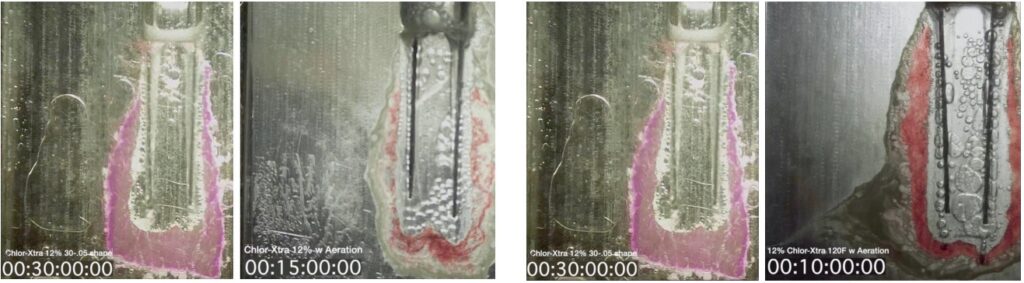
From a 40-minute time to dissolve the pulp analog with 6% NaOCl EndoVac irrigation (much of that time spent unclogging the EV needles), dissolution times were progressively shortened: 40 minutes to 30 minutes simply by reversing the direction of fluid flow, simultaneously eliminating the clogging problem inherent to using irrigation needles as vacuum pipes; 30 minutes reduced to 20 minutes by increasing the concentration of the NaOCl solution from 6% to 12% or by heating the solution to 109º F, and the dog-bites-man story of how simply aerating the solution halved the time to dissolution as air bubble cavitation exploding out the ends of the catheters imparting significant shear forces throughout the length of the canal.6
Applying all variables to shorten the time
Finally, I did a block test combining all four of those factors — concentration, the direction and volume of fluid flow, temperature, and aeration (Figure 9) — bringing the time to digest all the way through the isthmus pulp analog down to 10 minutes. This led to joining forces with Vista Dental to develop what we call the multi-canalar PulpSucker (PS) Closed-System Vacuum-Drawn Irrigation System (Figure 10).

Conclusion
This new irrigation system and method has the following advantages:
- PS Irrigation supports MIE canal shapes and single visit RCT for all cases.
- It is multi-canalar and works in all 1-5 canals simultaneously.
- It takes 2-4 minutes of hands-on to stage.
- It takes 8-15 minutes of hands-off irrigation run time.
- Vacuum-drawn irrigation with 8% NaOCl is 100% safe.
- There are no capital costs; no maintenance costs.
- These are single-use, completely disposable devices.
Besides endodontic irrigation, Dr. L. Stephen Buchanan educates colleagues on a variety of other topics. Read more about him in this Educator Profile: https://endopracticeus.com/l-stephen-buchanan-dds/
Author Info
 L. Stephen Buchanan, DDS, FICD, FACD, Dipl. ABE, was valedictorian of his class at the University of the Pacific School of Dentistry and completed the Endodontic Graduate program at Temple University in Philadelphia, Pennsylvania, in 1980. Dr. Buchanan began pursuing 3D-anatomy research early in his career, and in 1986, he became the first person in dentistry to use micro CT technology to show the intricacies of root structure. In 1989, he established Dental Education Laboratories and subsequently built a state-of-the-art teaching laboratory devoted to hands-on endodontic instruction, where he continues to teach today. Through Dental Education Laboratories, he has lectured and conducted participation courses around the world, published numerous articles, and produced an award-winning video series, “The Art of Endodontics.” In addition to his activities as an educator and practicing clinician, Dr. Buchanan holds a number of patents for dental instruments and techniques.
L. Stephen Buchanan, DDS, FICD, FACD, Dipl. ABE, was valedictorian of his class at the University of the Pacific School of Dentistry and completed the Endodontic Graduate program at Temple University in Philadelphia, Pennsylvania, in 1980. Dr. Buchanan began pursuing 3D-anatomy research early in his career, and in 1986, he became the first person in dentistry to use micro CT technology to show the intricacies of root structure. In 1989, he established Dental Education Laboratories and subsequently built a state-of-the-art teaching laboratory devoted to hands-on endodontic instruction, where he continues to teach today. Through Dental Education Laboratories, he has lectured and conducted participation courses around the world, published numerous articles, and produced an award-winning video series, “The Art of Endodontics.” In addition to his activities as an educator and practicing clinician, Dr. Buchanan holds a number of patents for dental instruments and techniques.
Disclosure: Dr. Buchanan is a stockholder of Sonendo; he is the inventor and owner of the IP associated with the closed-system, negative pressure, positive outflow irrigation (PulpSucker) device described in this article, and he is PlanB Dental’s Clinical Director.
References
- Hess W, Zurcher E, Dolamore WH. The Anatomy of the Root Canals of the Teeth of the Permanent Dentition. London: J. Bale Sons and Danielsson; 1925.
- Nixdorf DR, Law AS, John MT, Sobieh RM, Kohli R, Nguyen RH; National Dental PBRN Collaborative Group. Differential diagnoses for persistent pain after root canal treatment: a study in the National Dental Practice-based Research Network. J Endod. 2015;41(4):457-63.
- Retamozo B, Shabahang S, Johnson N, Aprecio RM, Torabinejad M. Minimum contact time and concentration of sodium hypochlorite required to eliminate Enterococcus faecalis. J Endod. 2010;36(3):520-3.
- Schoeffel GJ. The EndoVac method of endodontic irrigation: Part 2—efficacy. Dent Today. 2008;27(1):82,84,86-87.
- Haapasalo M, Wang Z, Shen Y, Curtis A, Patel P, Khakpour M. Tissue dissolution by a novel multisonic ultracleaning system and sodium hypochlorite. J Endod. 2014;40(8):1178-81.
- Buchanan LS. Closed System Negative Pressure Endodontic Irrigation: A Serious Inflection Point in Root Canal Cleaning. Dent Today. April 2020. https://www.dentistrytoday.com/endodontics/10666-closed-system-negative-pressure-irrigation-a-serious-inflection-point-in-root-canal-cleaning
