CE Expiration Date:
CEU (Continuing Education Unit): Credit(s)
AGD Code:
Educational aims and objectives
This article aims to demonstrate how a challenging root canal anatomy in a maxillary molar (UR6) was successfully negotiated using a methodical approach and reciprocating nickel-titanium instruments.
Expected outcomes
Endodontic Practice US subscribers can answer the CE questions by taking the quiz to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can:
- Recognize when the use of straight-line access is advisable.
- Identify tools with which to estimate working length.
- Recognize some possible techniques to establishing a glide path.
- Realize the essential component of the development of a reproducible glide path.
- Realize that in some patients micro-cracking of the root dentin can be induced during mechanical preparation.
Dr. John Rhodes shares his methodical approach to a necrotic tooth and periapical periodontitis.
Dr. John Rhodes demonstrates a methodical approach using reciprocating nickel-titanium instruments
Curved and sclerosed canals can raise difficulties for the operator during root canal treatment resulting in iatrogenic errors. In this case, challenging root canal anatomy in a maxillary molar (UR6) was successfully negotiated using a methodical approach and reciprocating nickel-titanium instruments.
Clinical examination
A 56-year-old man was referred for root canal treatment of his UR6 after his general dentist had been unable to locate or negotiate sclerosed canals in the painful tooth. Intraorally, there were no swelling, sinus tracts, visible cracks, or increased periodontal pocketing. The tooth was restorable, but the existing amalgam restoration was defective. The tooth was nonvital to sensitivity testing with Endo-Ice® (Coltene).
Radiographic assessment using a paralleling periapical radiograph (Rinn, Dentsply Sirona) showed a large amalgam restoration distally with poor marginal integrity. There was evidence of access cavity preparation and removal of dentin overlying the disto-buccal (DB) canal. The DB and palatal canals appeared patent, but the mesio-buccal (MB) canals had not been located or negotiated, and the MB root was significantly curved. There was evidence of periapical radiolucency. There were no discernible signs of periodontal disease or gross caries.


Diagnosis
A necrotic UR6 associated with periapical periodontitis.
Treatment options
Sensible treatment options in this case include:
- Nonsurgical root canal treatment, followed by placement of a cusp-coverage restoration
- Extraction only or replacement with an implant or bridge
- Extraction and replacement with an implant should be feasible but may require bone augmentation.
The natural tooth was eminently restorable, and a good root filling complimented with a well-fitting crown could be expected to function as well as an implant-supported crown for significantly less cost and surgery time (Torabinejad, et al., 2007; Hannahan and Eleazer, 2008; Pennington, et al., 2009).
Treatment
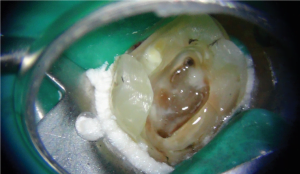
After discussing all the available options, the patient decided to have UR6 root filled. Nonsurgical root canal treatment was planned for a single visit. Following profound local anesthesia with articaine (Septodont), single tooth isolation was achieved with rubber dam and a No. 14 clamp. The existing restoration and caries were completely removed and the pulp floor refined with a Tungsten Carbide LN bur (Dentsply). A size 2 bur was used under the operating microscope to trough along the isthmus from MB1, which revealed a further two orifices (MB2 and MB3).
Straight-line access
Straight-line access is advisable when using rotary or reciprocating instruments. Removing calcified material from the coronal aspect makes transition deeper into the canal system easier, reduces stress on instruments, and allows rapid penetration of irrigant into the canal earlier during preparation. (Berruti, et al., 2004)
The orifice of each canal was explored to a depth of a few millimeters with a size 6 and 10 FlexoFile® (Dentsply Sirona) and then flared with a ProTaper® SX (Dentsply Sirona) instrument, brushing against the bulkiest wall of the canal and working to a depth approximately half the canal length as estimated from the preoperative radiograph. Thorough irrigation with 3% sodium hypochlorite was used throughout to remove debris. It was apparent that the MB2 communicated with the MB1, and therefore, it would not be necessary to enlarge this further.



Working-length estimation
All root lengths were estimated with a multi-frequency apex locator (Elements™ Diagnostics Unit, SybronEndo) and a size 6 FlexoFile with a small amount of Glyde™ (Dentsply) on the instrument. As consistent and steady zero readings were obtained, a diagnostic radiograph was not deemed necessary.
Establishing a glide path
The buccal canals were fine, and initially only a size 6 FlexoFile could be passed to the working length after coronal flaring. With a watch-winding action, this was enlarged to a size 10 FlexoFile using copious irrigation with 3% sodium hypochlorite. Once at the working length, the instrument was manipulated with small amplitude (2 mm-3 mm) vertical movements until it would reproducibly pass to the working length. This was particularly relevant in the DB canal, which had an acute curve in the apical tip. The working length was reconfirmed with the apex locator. A small WaveOne® Gold (Dentsply Sirona) reciprocating instrument was then used to enlarge the preliminary glide path to the full working length. This instrument has an average taper of 7% and a tip size 20.
WaveOne Gold instruments have a reciprocating action and have to be used in a dedicated electric motor. In this case, the X-Smart iQ cordless motor was used, which is controlled from a dedicated app on an iPad®. The app records and displays real-time torque monitoring, so if excess stress is incurred, the instrument auto-reverses with visual and audible warnings.
Preparation and tapering
Rapid tapering of the primary root canals was completed with WaveOne Gold (Dentsply Sirona) instruments, always working through a puddle of sodium hypochlorite on the pulp floor and patency confirmed with a size 10 FlexoFile. A single Primary WaveOne Gold instrument (average taper 7% and tip size 25) was used in all canals apart from the palatal, which was finished using a medium WaveOne Gold (average taper 6% and tip size 35).
Disinfection
A heated 3% solution of sodium hypochlorite was used to disinfect the prepared root canals. This was agitated using a freely vibrating Irrisafe™ tip (Satelec) inserted 2 mm from the working length and an EndoActivator® (Dentsply) with a Red tip using a pumping action.
Obturation
The case was obturated using a vertically compacted gutta-percha technique with heated pluggers, AH Plus® sealer (Dentsply Sirona), and Obtura (Obtura Spartan) thermo-plasticized gutta percha to backfill.
Coronal seal
The pulp floor and coronal aspect of the root canals were sealed with Smart Dentin Replacement (SDR – Dentsply Sirona) a bulk fill, flowable composite (this material will cure to a depth of 4 mm in bulk sections). The tooth was then temporized with resin modified glass ionomer (Fuji IX®). The general dental practitioner would complete restoration with a core and full coverage crown. Postoperative paralleling radiographs were exposed at two angles to confirm a homogenous seal. Review was scheduled for 6 months.
Discussion
The risk of blocking the canal during preparation is probably greater when the canal is fine or sclerosed because rotary or reciprocating instruments machine a comparatively greater surface area of the root canal wall and therefore create more dentin chips. The chips and smear can block the canal or pack into the flutes of the instrument and increase the risk of tip fracture. The volume of available irrigant is also reduced resulting in smear “clumping.” Copious irrigation during preparation and recapitulation with a fine file can be used to avoid this happening.
WaveOne Gold instruments are manufactured with heat-treated M-wire. In-house testing by Dentsply Sirona has shown that cyclic fatigue resistance has been improved by 50% compared with WaveOne and 100% more than most standard rotary systems. WaveOne Gold instruments are 80% more flexible than WaveOne.
Despite superior metallurgy, it is essential to create a reproducible glide path for nickel-titanium instruments to follow (Nahmias, et al., 2013; Kubde, 2012). The glide path reduces the chance of instrument fracture as a result of cyclic or torsional fatigue or when the tip becomes locked in the canal. (Sattapan, et al., 2000; Patiño, et al., 2005; Plotino, et al., 2009).
Flexible stainless steel instruments such as FlexoFiles can be used to scout the canals and establish patency followed by a narrow taper rotary or reciprocating instrument to create the glide path. In this case, FlexoFiles and a small WaveOne Gold instrument were used. The ProGlide® (Dentsply Sirona) is a rotary instrument that has been designed specifically for this purpose and has been shown to be one of the most efficient means of preparing a glide path (Van der Vyver, 2015).
There is evidence that micro-cracking of the root dentin can be induced during mechanical preparation (Yoldas, et al., 2012). This appears to be more prevalent with rotary techniques and when larger sizes or tapers are used. Generally, the canals should be tapered sufficiently to allow adequate irrigant penetration but avoid excessive dentin removal (Liu, et al., 2011). WaveOne Gold instruments are operated in a reciprocating motion, which reduces stress. They have progressive tapers, but the average apical taper has been reduced from equivalent WaveOne instruments, and the manufacturer has introduced an intermediate size medium file with tip size 35.




Mechanical preparation alone can reduce the bacterial load in an infected root canal (Byström and Sundqvist, 1981), but sodium hypochlorite in a concentration of at least 1% is required to kill any remaining bacteria (Byström and Sundqvist, 1983). Bacteria in a necrotic root canal system such as this case are present in planktonic form and as a complex biofilm in which bacteria are surrounded by matrix on the walls of the canals and can be difficult to remove.
Irrigants must therefore be agitated to break up these bacterial aggregations. It is possible to achieve acoustic microstreaming when an ultrasonic file oscillates freely in the root canal (Ahmad, et al., 1987), and the forces created by the turbulence may disrupt biofilm. Passive ultrasonic irrigation (PUI) utilizes a small file oscillating freely in the root canal to induce acoustic microstreaming, and in this case, PUI and agitation with the EndoActivator were used. Compared with traditional syringe irrigation, PUI removes more organic tissue, planktonic bacteria, and dentin debris from the root canal (Burleson, et al., 2007; van der Sluis, et al., 2007).
It can be difficult to ensure adequate irrigant exchange at the apex of fine, long, or highly curved canals. The primary canals must be sufficiently tapered to allow sufficient volume of irrigant to be introduced into the root canal system. Conservative tapering of the canal is generally not a problem with modern nickel- titanium systems.
The chelating agent 17% EDTA is sometimes used as a final rinse during irrigation (Byström and Sundqvist, 1985). It is used to remove smear and has a positive benefit on outcome in retreatment cases; however, this does not seem to be the case with primary treatment (Ng, et al., 2011).
In a two-visit approach, the canals are medicated after preparation and disinfection with calcium hydroxide for 7 days. This has been shown to be an effective means of producing bacteria-free canals (Byström, Claesson, Sundqvist, 1985; Sjögren, et al., 1991). However, more recently, Peters, et al. (2002), showed that calcium hydroxide and sterile saline slurry limits but does not totally prevent regrowth of endodontic bacteria. Hargreaves (2006) in a systematic review of the literature reported that multiple visits with calcium hydroxide treatment did not improve upon clinical outcome, and there was a minimal level of evidence for considering one versus two appointments in nonsurgical endodontics. Indeed, meta-analysis has shown that a single-visit approach (as used by many endodontists) has no bearing on prognosis, outcome, or postoperative pain (Ng, et al., 2011). This case was therefore completed in a single visit.
Conclusion
In this case, curved and sclerosed canals in a maxillary molar were managed using WaveOne Gold instruments. The development of a reproducible glide path was essential. The operator should not be put off by the preoperative radiographic appearance or lack of canal definition on a CBCT image. However, often the canals are not as fine as they seem, so by using a methodical approach to preparation, these anatomical challenges can be overcome.
Dr. Rhodes has demonstrated his methodical approach to endodontics in another article, “Problem-solving endodontics.”
https://endopracticeus.com/clinical-articles/problem-solving-endodontics-2/.
References
- Ahmad M, Pitt Ford TJ, Crum LA. Ultrasonic debridement of root canals: acoustic streaming and its possible role. J Endod. 1987;13(10):490-499.
- Berutti E, Negro AR, Lendini M, Pasqualini D. Influence of manual preflaring and torque on failure rate of the ProTaper rotary instruments. J Endod. 2004;30(4):228-230.
- Burleson A, Nusstein J, Reader A, Beck M. The in vivo evaluation of hand /rotary/ultrasound instrumentation in necrotic human molars. J Endod. 2007;33(7):782-787.
- Byström A, Sundqvist G. Bacteriologic evaluation of the efficacy of mechanical root canal instrumentation in endodontic therapy. Scand J Dent Res. 1981;89(4):321-328.
- Byström A, Sundqvist G. Bacteriologic evaluation of the effect of 0.5 percent sodium hypochlorite in endodontic therapy. Oral Surg Oral Med Oral Pathol. 1983;55: 307-312.
- Byström A, Sundqvist G. The antibacterial action of sodium hypochlorite and EDTA in 60 cases of endodontic therapy. Int Endod J. 1985;18:35-40.
- Byström A, Claesson R, Sundqvist G. The antibacterial effect of camphorated paramonochlorophenol, camphorated phenol and calcium hydroxide in the treatment of infected root canals. Endod Dent Traumatol. 1985;1(5):170-75
- Hannahan JP, Eleazer PD. Comparison of success of implants versus endodontically treated teeth. J Endod. 2008;34(11):1302-11305
- Hargreaves KM. Single-visit more effective than multiple-visit root canal treatment. Evid Based Dent. 2006;7(1)13-14.
- Kubde R, Saxena A, Chandak M, Bhede R, Sundarkar P. Creating endodontic glide path: A short review. Int J Dent. 2012;4(1):40-41.
- Liu R, Kaiwar A, Shemesh H, et al. Incidence of apical root cracks and apical dentinal detachments after canal preparation with hand and rotary files at different instrumentation lengths. J Endod. 2011;39:129-132.
- Nahmias Y, Cassim I, Glassman G. Own the canal – the importance of a reproducible glide path. Oral Health. 2013;5:74-82.
- Ng YL, Mann V, Gulabivala K. A prospective study of the factors affecting outcomes of nonsurgical root canal treatment: part 1: periapical health. Int Endod J. 2011;44:583-609.
- Patiño PV, Biedma BM, Liébana CR, Cantatore G, Bahillo JG. The influence of manual glide path on the separation rate of NiTi rotary instruments. J Endod. 2005;31:114-116.
- Pennington MW, Vernazza CR, Shackley P, et al. Evaluation of the cost-effectiveness of root canal treatment using conventional approaches versus replacement with an implant. Int Endod J. 2009;42:874-883.
- Peters LB, van Winkelhoff AJ, Buijs JF, Wesselink PR. Effects of instrumentation, irrigation and dressing with calcium hydroxide on infection in pulpless teeth with periapical bone lesions. Int Endod J. 2002; 35, 13-21.
- Plotino G, Grande NM, Cordaro M, Testarelli L, Gambarini, G (2009). A review of cyclic fatigue testing of nickel-titanium rotary instruments. J Endod. 35: 1469-76.
- Sattapan B, Nervo GJ, Palamara JE, Messer HH. Defects in rotary nickel titanium files after clinical use. J Endod. 2000;26(3):161-165.
- Sjögren U, Figdor D, Spångberg L, Sundqvist G. The antimicrobial effect of calcium hydroxide as a short-term intracanal dressing. Int Endod J. 1991;24(3):119-125.
- Torabinejad M, Anderson P, Bader J, et al. Outcomes of root canal treatment and restoration, implant-supported single crowns, fixed partial dentures and extraction without replacement: a systematic review. J Prosthet Dent. 2007;98(4):285-311.
- van der Sluis LW, Versluis M, Wu MK, Wesselink PR. Passive ultrasonic irrigation of the root canal: a review of the literature. Int Endod J. 2007;40:415-426.
- Van der Vyver PJ, Paleker F, Jonker CH. Comparison of preparation times of three different rotary glide path instrument systems. S Afr Dent J. 2015;70(4):144-147.
- Yoldas O, Yilmaz S, Atakan G, Kuden C, Kasan Z. Dentinal microcrack formation during root canal preparations by different NiTi rotary instruments and the self-adjusting file. J Endod. 2012;38(20:232-235.
