Dr. Gregori M. Kurtzman explains why endodontic files and sealers can mean the difference between success and failure of endodontic treatment and how these new products, debuted by SS White, can make a difference.
Dr. Gregori M. Kurtzman describes the characteristics of new hand files and bioceramic sealer
Endodontic treatment has advanced over the past 4 decades. Instrumentation, traditionally performed utilizing hand files that were 02 in taper, led to potentially being unable to instrument canals easily and efficiently, as certain canals had greater tapers than the files available at the time. Filing was performed with a reciprocal motion which added to procedure inefficiency. The introduction of rotary files improved treatment efficiency. Tapers that more closely matched the shape of the canal and rotary motion with the file were able to clean and shape the canal better than reciprocal motion utilized with hand files. Additionally, hand files were fabricated with stainless steel which does not have the flexibility of NiTi rotary files. More flexible files can follow the canals’ curvature without overinstrumenting the canal when a curved canal is more pronounced.
Rotary NiTi files aid in maintaining as much native tooth structure as possible, especially in the coronal and cervical portion of the root by cleaning the canal walls without removing excess tooth structure following the canals’ natural anatomy and taper.
Obturating the canal system also has undergone advances in recent years. Traditional sealers, zinc oxide and eugenol (ZOE) or calcium hydroxide-based have been in use for many decades.
ZOE sealers are extremely sensitive to moisture in the canal system, which can inhibit their setting reaction. This can result in incomplete or inadequate sealing of the canal system. Studies have demonstrated a higher leakage than the other sealers.1 ZOE sealers, as they contain eugenol, have been shown to have potential toxic effects on surrounding tissues, especially if sealer is extruded apically during obturation. This can irritate the extra apical periodontal tissue causing an inflammatory response.2 ZOE sealers are also soluble in the presence of oral fluids or moisture, which can lead to the gradual loss of the sealer creating pathways for bacterial leakage and reducing the longevity of the seal.3
Calcium hydroxide-based sealers have been used due to their bactericidal nature and tissue healing properties. However, these sealers also have limitations related to their poor sealing ability and potential for gaps or shrinkage. This may lead to leakage and subsequent failure of the endodontic treatment.4 These sealers exhibit significant solubility in oral fluids that can lead to the gradual breakdown of the material, resulting in loss of the sealing function. Additionally, these types of sealers do not strongly adhere to dentin, which may lead to gaps or poor adaptation between the sealer and the canal walls. This lack of adhesion increases the likelihood of microbial leakage, potentially compromising the success of treatment.5
With those issues of traditional endodontic sealers, the shift was to a sealer type that is not affected by moisture during setting, is insoluble to eliminate potential leakage, and is bio-compatible if extruded apically. Bioceramic sealers met those expectations and originated in orthopedics in the 1970s for treatment of bone defects.6 Use in dentistry began a few decades ago, and use as an endodontic sealer was a natural transition related to its biocompatibility, bond to dentin, and insolubility once set.
The EXIMIA7™ file system
EXIMIA7™ endodontic files are designed with precision, flexibility, and durability to improve and simplify instrumentation of the canal system. These NiTi files are heat treated to increase resistance to cyclic fatigue and enhance the files’ strength and flexibility, minimizing shape memory for optimal precision. This also allows for extreme flexibility of the file in curved canals, reducing file shape memory, preserving canal anatomy, and limiting or eliminating over-instrumentation of the inner curve that may happen with stiffer files. Additionally, the files allow for instrumentation in challenging canal anatomy. The “controlled memory” of EXIMIA7™ files allows the file to return to its original shape after being bent during instrumentation in curved canals, thus maintaining the desired path in the canal.
The files have a parabolic cross section, maximizing the files’ cutting efficiency for smoother procedures. They have a 1mm maximum flute diameter that allows for minimally invasive preparation, preserving tooth structure in the critical cervical area of the root. A non-cutting tip on the files provides precise guidance and centering the files within the canal, aiding in eliminating file transportation away from canals’ true path or perforation of the lateral aspect of the root.
EXIMIA7™ files’ sharp cutting edges allow for efficient and smooth removal of debris and tissue from the canal, minimizing the risk of ledging or zipping. The constant taper with a variable pitch design improves cutting efficiency while reducing file binding, or potential file separation.
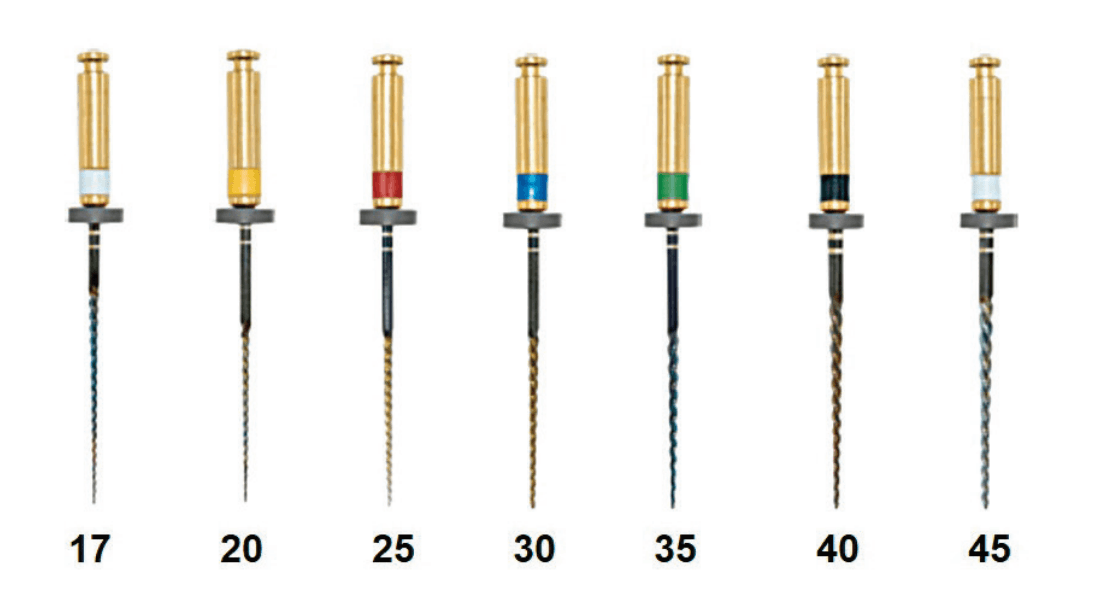
They are available in .04 and .06 constant tapers with an ISO tip size of 17-45 in available lengths of 21 mm, 25 mm, and 29 mm (Figure 1). The system additionally provides gutta-percha cones and paper points that match the files’ taper and size to allow single cone obturation, allowing the fitted cone to press sealer into the adjacent canal anatomy (Figures 2 and 3). The gutta-percha cones and paper points have length markings on them to aid in assuring working length (WL) is achieved when drying the canals and during obturation.

PURE-Ca-SEAL™ bioceramic sealer
PURE-Ca-SEAL™, an FDA-approved premixed bioceramic endodontic sealer, releases calcium ions to form mineralized tissue within the canal system and apically. The alkaline pH and low solubility of the sealer creates a hermetic seal within the canal system, making the environment within the canal system and at the apical orifice inhospitable for bacterial growth. In cases of non-communicating internal resorption, the high pH of PURE-Ca-SEAL™ neutralizes the acidic environment, assisting in halting the progression of the resorption.

This ready-to-use formulation simplifies the obturation procedure (Figure 4), resulting in less chair time and increased patient comfort. PURE-Ca-SEAL™ can be utilized with any obturation technique, including those that involve heat. The resin-free formula features a small particle size, providing a thin film thickness and excellent flow characteristics.7 Unlike ZOE and calcium hydroxide-based sealers, its hydrophilic properties are ideal for setting in a moist environment. Additionally, it is well accepted by the tissue should any sealer be extruded apically.8
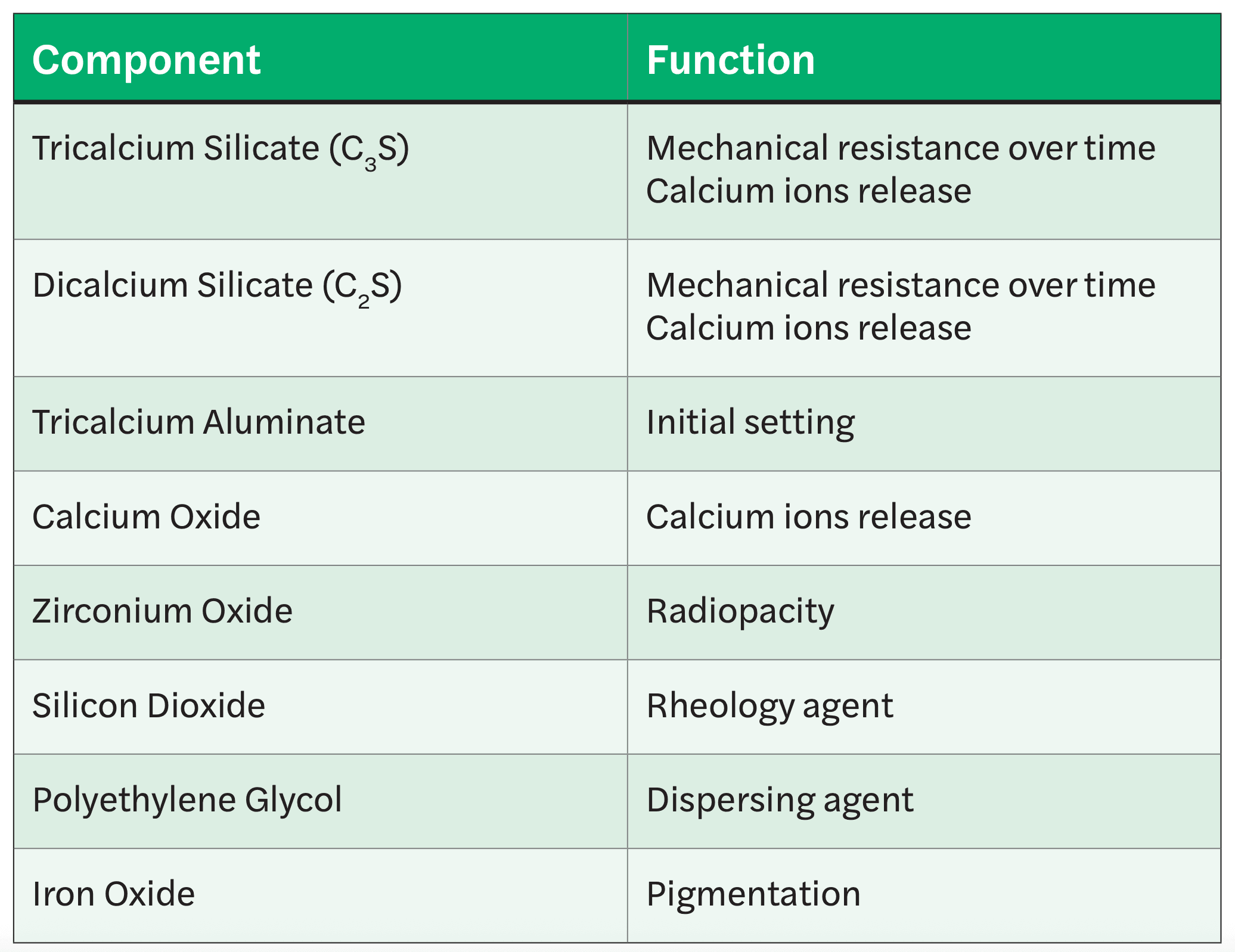
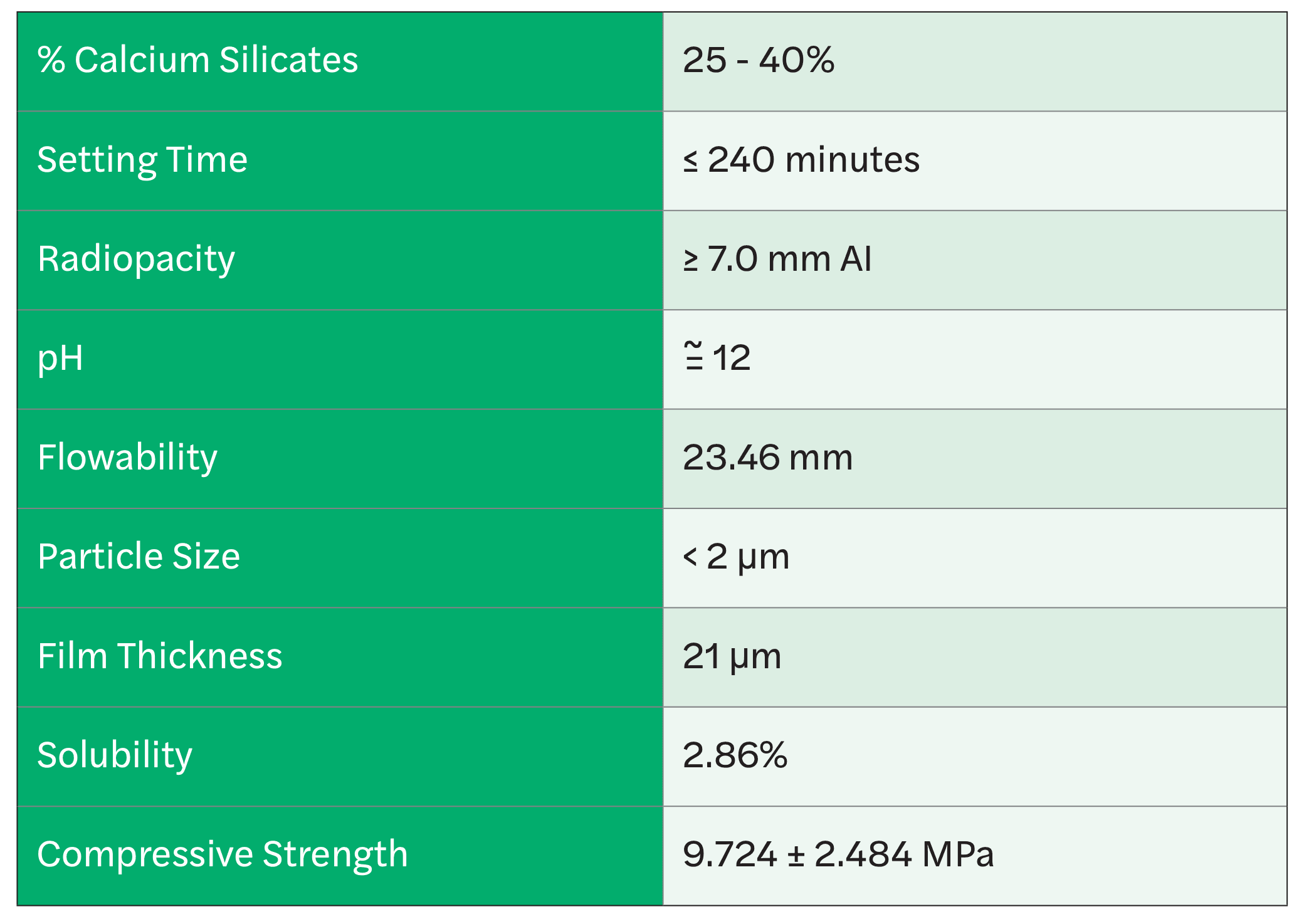
The components of the sealer provide high radiopacity, mechanical resistance to calcium ion release, and other factors enhancing clinical results (Figure 5). The sealer has a setting time of ~240 minutes, good flowability, and high compressive strength once set (Figure 6). The sealers’ mechanisms of action are closely associated with contact with tissue moisture and fluids. After the calcium oxide present in the sealer comes into contact with the water present in the dentin tubules, calcium hydroxide is formed which interacts with the fluids, dissociating in calcium ion and hydroxyl. The hydroxyl ions are responsible for the increase in pH promoting its bactericidal action.9 The released Ca2+ ions react with CO2 from the bloodstream, forming calcium carbonate (calcite), and extra-cellular matrix rich in fibronectin is secreted attracted by calcite, triggering formation of hard tissue.
Case report
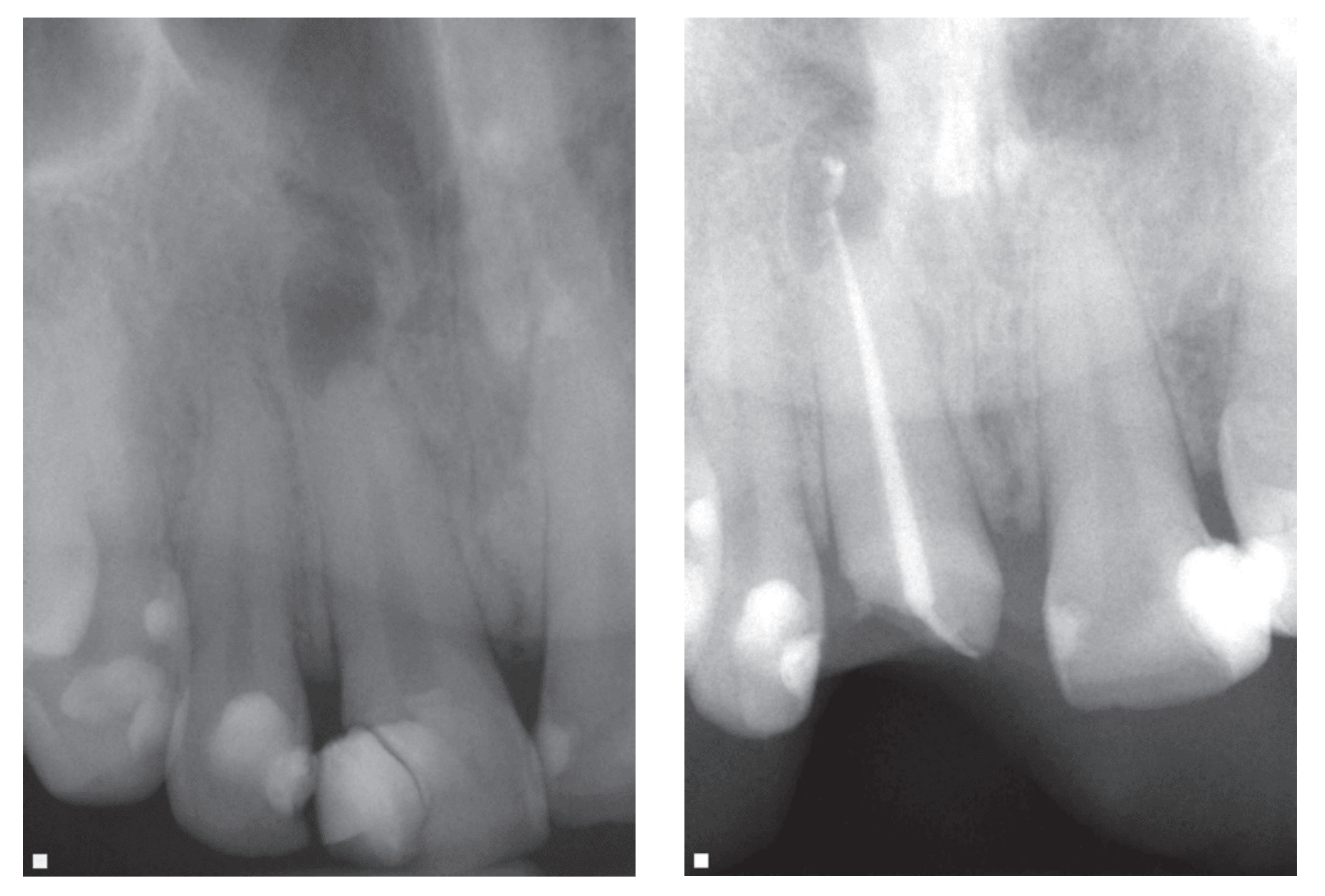
A 32-year-old male patient presented with a complaint of a loose filling on the maxillary right central incisor (Tooth No. 8). Examination noted a large composite filling that was loose on the tooth. A periapical radiograph showed a large periapical lesion on the right central incisor (Figure 7). The pulp of the tooth appeared larger than the adjacent central incisor, and when questioned, the patient indicated previous trauma to the tooth. He further indicated no hot, cold, or biting sensitivity on the tooth. The tooth tested negative for percussion as well as when tested with Endo-Ice® (Coltene Dental, Cuyahoga Falls, Ohio) or heat. The patient was advised that endodontic treatment was indicated as the pulp was non-vital and had an apical lesion. He indicated he would speak to his spouse about the purpose of treatment.
The patient returned several weeks later related to the old filling falling out of the tooth and fracturing a portion of the coronal. The patient indicated he was still not having any pain or sensitivity in the tooth. Local anesthetic was administered via infiltration into the vestibule adjacent to the tooth to be treated with 1 carpule 4% Septocaine with 1:200,000 epi (Septodont, New Castle, Delaware). A rubber dam was placed with rubber dam clamps on teeth Nos. 6 and 11. Access was created on tooth No. 8 with a 330-carbide bur in a high-speed handpiece. A size 25 hand file was introduced into the canal to the estimated working length (18 mm) as measured on the initial radiograph and verified with an apex locator. No bleeding was noted in the canal, confirming that the pulp was non-vital.
The canal was instrumented to a size 35 with a 04 taper EXIMIA7™ rotary file. The canal was irrigated with a 2.5% NaOCl solution followed by a 17% EDTA solution while using the last rotary file to aid in distributing the irrigation into the canal system. The canal was dried with paper points matching the final file size of 35 with a 04 taper. PURE-Ca-SEAL™ bioceramic sealer was dispensed on a pad, and a gutta-percha cone matching the final file (35 with 04 taper) was coated with the sealer and introduced into the canal to WL. The excess cone coronally was cut off with a heated instrument at the canal orifice. A periapical radiograph was taken (Figure 8). The radiographs demonstrated complete obturation of the canal with slight extrusion of sealer at the apical. Also noted was slight external resorption at the apical related to the lesion. The patient was scheduled for placement of a fiber post with composite core and a full crown.
Conclusion
Endodontics is a 2-part process, encompassing instrumentation and obturation. Success requires both parts to be performed well. The EXIMIA7™ file system provides improved canal instrumentation with flexibility of the files to follow canal anatomy while aiding in preserving root structure to improve tooth longevity. When combined with a bioceramic sealer like PURE-Ca-SEAL™ a predictable obturation can be achieved that is insoluble to oral fluids, antibacterial, and well tolerated apically should any sealer be extruded during obturation.
SS White knows about endodontic files and sealers. Read more about what their team would use if their loved one needed a root canal. https://endopracticeus.com/industry-news/loved-one-needs-root-canal/
 Gregori Kurtzman, DDS, is in private general dental practice in Silver Spring, Maryland. He is a former Assistant Clinical Professor at University of Maryland in the department of Restorative Dentistry and Endodontics and a former AAID Implant Maxi-Course assistant program director at Howard University College of Dentistry. He has lectured internationally on the topics of restorative dentistry, endodontics and implant surgery, removable and fixed prosthetics, and periodontics. He has over 900 published articles, as well as several ebooks and textbook chapters. He can be reached at dr_kurtzman@maryland-implants.com.
Gregori Kurtzman, DDS, is in private general dental practice in Silver Spring, Maryland. He is a former Assistant Clinical Professor at University of Maryland in the department of Restorative Dentistry and Endodontics and a former AAID Implant Maxi-Course assistant program director at Howard University College of Dentistry. He has lectured internationally on the topics of restorative dentistry, endodontics and implant surgery, removable and fixed prosthetics, and periodontics. He has over 900 published articles, as well as several ebooks and textbook chapters. He can be reached at dr_kurtzman@maryland-implants.com.
Disclosure: Dr. Kurtzman is a key opinion leader for SS White.
- Hakke Patil A, Patil AG, Shaikh S, Bhandarkar S, Moharir A, Sharma A. Comparative Evaluation of the Sealing Ability of Mineral Trioxide Aggregate (MTA)-Based, Resin-Based, and Zinc Oxide Eugenol Root Canal Sealers: An In Vitro Study. 2024 Jan 13;16(1):e52201. doi: 10.7759/cureus.52201.
- Huumonen S, Lenander-Lumikari M, Sigurdsson A, Ørstavik D. Healing of apical periodontitis after endodontic treatment: a comparison between a silicone-based and a zinc oxide-eugenol-based sealer. Int Endod J. 2003 Apr;36(4):296-301. doi: 10.1046/j.1365-2591. 2003.00651.x.
- Poggio C, Arciola CR, Dagna A, Colombo M, Bianchi S, Visai L. Solubility of root canal sealers: a comparative study. Int J Artif Organs. 2010 Sep;33(9):676-81. doi: 10.1177/ 039139881003300914.
- Desai S, Chandler N. Calcium hydroxide-based root canal sealers: a review. J Endod. 2009 Apr;35(4):475-80. doi: 10.1016/j.joen.2008.11.026. Epub 2009 Feb 26.
- Lee KW, Williams MC, Camps JJ, Pashley DH. Adhesion of endodontic sealers to dentin and gutta-percha. J Endod. 2002 Oct;28(10):684-8. doi: 10.1097/00004770-200210000-00002.
- Daculsi G. History of Development and Use of Bioceramics and Biocomposites. In: Antoniac I, ed. Handbook of Bioceramics and Biocomposites. Springer, Cham;2016. https://doi.org/10.1007/978-3-319-09230-0_2-2.
- Tanomaru-Filho M, Esteves Torres FF, Pinto JC, Guerreiro Tanomaru JM, Pereira MC, de Souza PFF. Flow, Filling Ability and Apical Extrusion of New Calcium Silicate-Based Sealers: A Micro-Computed Tomographic Study. Dental Oral Biology and Craniofacial Research. June 2020;1-6. 10.31487/j.DOBCR.2020.03.04.
- Alves Silva EC, Tanomaru-Filho M, da Silva GF, Delfino MM, Cerri PS, Guerreiro-Tanomaru JM. Biocompatibility and Bioactive Potential of New Calcium Silicate-based Endodontic Sealers: Bio-C Sealer and Sealer Plus BC. J Endod. 2020 Oct;46(10):1470-1477. doi: 10.1016/j.joen.2020.07.011. Epub 2020 Jul 17.
- Viana FLPP. Antimicrobial activity of biocerose endodontic cements in front of enterococcus faecalis in biofilm – in vitro study. 2019. 46 f. Dissertation (Master in Dentistry) – Faculty of Pharmacy, Dentistry and Nursing, Federal University of Ceará, Fortaleza, 2019.
Stay Relevant With Endodontic Practice US
Join our email list for CE courses and webinars, articles and more..
